
One of the most popular and recent uses of SARM occurs during the PCT period, a critical period following an anabolic steroid or prohormone cycle.
To see and understand why, you need to look at what happens after your cycle and during the PCT period.
Closing the cycle
Taking an anabolic compound of androgens, whether steroids or prohormones, natural hormonal production This affects the body.
The body detects an abundance of androgens, thereby signaling the hypothalamus to reduce the secretion of GnRH .
This, in turn, causes a decrease in the secretion of LH and FSH by the pituitary gland, which in turn signals the Leydig cells in the testes to decrease or stop the production of testosterone.
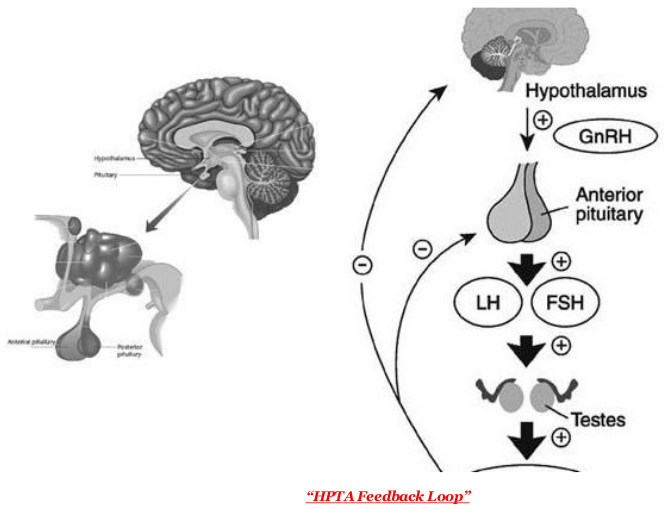
– This negative feedback loop causes testicular atrophy or contraction during use. –
The role of PCT – post cycle therapy
The goal of PCT (post cycle therapy) is to quickly normalize hormone production. endogenous, and then signal the body to resume normal testosterone production.
The most common and effective compounds used to achieve this are SERM (Selective Estrogen Receptor Modulators) Nolvadex (Tamoxifen Citrate) and Clomid (Clomiphene Citrate). Nolvadex and Clomid are used immediately after a cycle to get homeostasis (normal hormone levels) at a faster rate. However, even with Nolvadex / Clomid, the recovery period for hormone levels is long. It is during this period of the PCT that the loss of muscle mass and strength occurs.
Ostarine in the PCT
This is the moment when SARMs like Osstarine are offering their benefits. Ostarine binds to the musculoskeletal androgen receptor, continuing to activate the androgen receptor, while nolvadex and clomid return natural testosterone production to normal.
As a result of this continued activation of receptors in muscles, loss of muscle mass and strength during PCT is minimized, and most users also report increases in strength.

Food Consumption
Another very important factor in PCT is CALORIES . As mentioned earlier, the endocrine system does not function optimally after a cycle.
The body tends to maintain homeostasis after a cycle in a very dense state where it has reached an “unusual” amount of mass. To maintain this state (especially when you are in a suboptimal hormonal environment), calorie intake must equal or exceed what is present during the cycle.
Knowing this, users may be reluctant to consume so many calories when they are no longer in cycle, also because of the risk of fat accumulation that can occur with high calorie intake.
The anabolic and destructive effects of ostarine allow the user to maintain calorie stability. during PCT prevents fat gain.
– But does Osstarine suppress? –
Ostarina has been designed to minimize endogenous testosterone suppression. However, some users report that at doses in excess of 25 mg ostarine, it can cause some mild suppression. Therefore, it would be unwise to use ostarine at these doses as the only form of PCT.
However, when using ostarine in combination with SERMs such as nolvadex (tamoxifen) or clomid (clomiphene), agonism in the pituitary and hypothalamus nolvadex / clomid can compensate possible slight suppression of ostarine.
Thus, nolvadex and clomid will help to obtain normal endogenous testosterone levels, while ostarine has the benefits of androgen receptor activity.
PCT Dosage
The most common dosing protocol appears to be a higher intake followed by a lower dose during the rest of the PCT period. A typical dosing protocol is as follows: 25 mg for the first 1-2 weeks of PCT, then switch to 12.5-15 mg for the rest of the PCT (4-5 weeks).
Since Osstarin has a half-life of approximately 24 hours, the dose should only be taken once a day.
Starting at a higher dose for the first 1-2 weeks, it is recommended to use Nolvadex / blood levels. Clomid and their subsequent effects are not immediate. While natural hormone levels are still low at the beginning of the PCT period, a higher dose of ostarine will provide increased activation of androgen receptors in muscle tissue in the absence of endogenous hormones.
Of course, if you are still concerned about the risk of suppression, even with SERMs. 10-12.5mg during the PCT period will provide the benefits of an androgen receptor agonist without suppressing the effect.
Some users report extending this period even further, decreasing the dose to 5mg over 5-8 weeks.

So, in conclusion, it should be noted that while high doses of SARMs may cause mild suppression, concomitant use of selective estrogen receptor modulators such as nolvadex / clomid compensates for this. Therefore, the use of SARMs, in particular ostarine with its lack of androgenic effects, is a positive choice for maintaining or even increasing gain and performance after an anabolic steroid / prohormone cycle.

