Let’s pause for a moment to think about the side effects, which are arguably the worst of the short term. As for the sexual ones, you think they are an advantage.
We say yes, but I must remember that an increase in libido, if not satisfied (Freud teaches …), can transform into other types of drives, up to before the crime. Finally, remember that an initial increase inevitably follows a decrease after suspension for the physiological reasons explained above. When it comes to the impact on aggression, I remember that they often wish bodybuilders or powerlifters to go to the gym more busy to lift huge weights. I do not deny that it is effective, but at what cost! If you really feel that you need the extra nerve to gain weight, it can mean many things, for example:
Dealing with these anabolic psychological “disorders” is absurd; It is better to act at the root of the problem, eliminate harmful causes and learn to control your mind, how to control your muscles. For all this, there are special methods (self-hypnosis, autogenous training).
As for other anabolic steroids, it should be said that their effect on libido and aggression, apparently, is associated with the degree of androgenicity: from my own experience, I have even seen that few androgenic foods (eg winstrol) tend to reduce libido in some subjects when used alone: however, this should not be dependent on a decrease in gonadotropins.
Now let’s look at some other effects not necessarily related to the androgenicity of foods .
Between this we remember:
Let’s pause for a moment to think about the side effects, which are arguably the worst of the short term. As for the sexual ones, you think they are an advantage.
We say “yes”, but I must remember that an increase in libido, if it is not satisfied (Freud teaches …), can be transformed into other types of drives, up to a crime. Finally, remember that an initial increase inevitably follows a decrease after suspension for the physiological reasons explained above. When it comes to the impact on aggression, I remember that they often wish bodybuilders or powerlifters to go to the gym more busy to lift huge weights. I do not deny that it is effective, but at what cost! If you really feel like you need the extra nerve to gain weight, it can mean many things, for example:
- You are probably mildly overtrained or the routine is boring and unproductive;
- You have other psychological problems;
- You are not made for this sport;
- In all the above cases, you are still wrong.
Dealing with these anabolic psychological “disorders” is absurd; It is better to act at the root of the problem, eliminate harmful causes and learn to control your mind, how to control your muscles. There are special methods for all this (self-hypnosis, autogenous training). As for other anabolic steroids, it should be said that their effect on libido and aggression seems to be related to the degree of androgenicity: from my own experience, I have even seen that few androgenic products (e.g. winstrol) tend to even decrease libido in some subjects when used alone: however, this should not be dependent on a decrease in gonadotropins.

Now let’s look at some other effects, not necessarily related to the androgenicity of foods. These include:
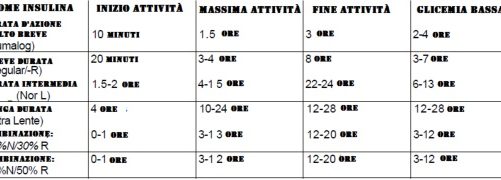
- Altered blood sugar levels. Androgenic anabolic agents can increase insulin sensitivity, this usually does not lead to hypoglycemia, but to a possible increase in its effects, that is, increase in fat, water retention, etc. These phenomena seem to be more pronounced in drugs that are sensitive to peripheral aromatization.
- Modification of blood lipids (fats) . I will dwell on this aspect for a moment, among the latter to be discovered. Androgenic-anabolic substances tend to reduce triglyceride levels by reducing the concentration of very low density lipoproteins (VLDL): this effect, in itself positive, is inherent in some derivatives of the progestogen nortestosterone, partly the same durabolin, oxandrolone, etc. However, over the past 5 years, they have been found to dramatically lower high-density lipoprotein levels, which carry the “good” portion of cholesterol (that is, HDL, which is the one that clears the arteries), and instead raise cholesterol levels associated with LDL lipoproteins (which Clog the arteries, predisposing to atherosclerosis).
And think that they were even used to treat hypertriglyceridemia! The effect does not depend on the dose, but, by blocking a certain enzymatic pathway, it appears already in small doses, and sometimes within just 2 days. All drugs, regardless of their characteristics (androgenicity, aromatization), seem to share it. Now, this side effect (along with the hypertension, which I will continue about) is the most dangerous mean to me. Without noticing that nothing (while acne and water retention become clearly visible), the arteries become blocked, It cannot be said that atherosclerosis affects all those who take anabolic drugs, but it is undoubted that the risk increases enormously, and not in a probabilistic way ( such as smoking – lung cancer), but much more direct, that is, associated with the duration of intake. What is usually the first sign of atherosclerosis in a relatively young subject? It is easy to say: death from a heart attack. In the following years, the manifestations, although very serious, become more treatable (with medication, surgery, etc.), but I think you all know what it means to suffer from the heart. Other complications occur at an older age (60-70 years) on the kidneys, brain, etc. Therefore, please do not say that “those who take anabolic are healthy like fish” or something like that: it seems as healthy as a fish, but his arteries are very likely to be destroyed, and would be curious to know if in middle age, especially when you stop exercising, I still feel so good.
Propensity for water retention and hypertension
Let’s pause for a moment to think about the side effects, which are arguably the worst of the short term. As for the sexual ones, you think they are an advantage.
We say yes, but I must remember that an increase in libido, if not satisfied (Freud teaches …), can transform into other types of drives, up to before the crime. Finally, remember that an initial increase inevitably follows a decrease after suspension for the physiological reasons explained above. When it comes to the impact on aggression, I remember that they often wish bodybuilders or powerlifters to go to the gym more busy to lift huge weights. I do not deny that it is effective, but at what cost! If you really feel that you need the extra nerve to gain weight, it can mean many things, for example:
Dealing with these anabolic psychological “disorders” is absurd; It is better to act at the root of the problem, eliminate harmful causes and learn to control your mind, how to control your muscles. For all this, there are special methods (self-hypnosis, autogenous training).
As for other anabolic steroids, it should be said that their effect on libido and aggression, apparently, is associated with the degree of androgenicity: from my own experience, I have even seen that few androgenic foods (eg winstrol) tend to reduce libido in some subjects when used alone: however, this should not be dependent on a decrease in gonadotropins.
Now let’s look at some other effects not necessarily related to the androgenicity of foods .
Between this we remember:
Let’s pause for a moment to think about the side effects, which are arguably the worst of the short term. Sexuals do you think they are an advantage.
We say yes, but I must remember that an increase in libido, if it is not satisfied (Freud teaches …), can be transformed into other types of drives, up to crime. Finally, remember that an initial increase inevitably follows a decrease after suspension for the physiological reasons explained above. When it comes to the impact on aggression, I remember that they often wish bodybuilders or powerlifters to go to the gym more busy to lift huge weights. I do not deny that it is effective, but at what cost! If you really feel like you need the extra nerve to gain weight, it can mean many things, for example:
- You are probably mildly overtrained or the routine is boring and unproductive;
- You have other psychological problems;
- You are not made for this sport;
- In all the above cases, you are still wrong.
Dealing with these anabolic psychological “disorders” is absurd; It is better to act at the root of the problem, eliminate harmful causes and learn to control your mind, how to control your muscles. There are special methods for all this (self-hypnosis, autogenous training). As for other anabolic steroids, it should be said that their effect on libido and aggression seems to be related to the degree of androgenicity: from my own experience, I have even seen that few androgenic products (e.g. winstrol) tend to even decrease libido in some subjects when used alone: however, this should not be dependent on a decrease in gonadotropins.
Now let’s look at some other effects, not necessarily related to the androgenicity of foods. These include:
- Altered blood sugar … Androgenic anabolic agents can increase insulin sensitivity, this usually does not lead to hypoglycemia, but to a possible increase in its effects, that is, increase in fat, water retention, etc. These phenomena seem to be more pronounced in drugs that are sensitive to peripheral aromatization.
- Modification of blood lipids (fats) . I will dwell on this aspect for a moment, among the latter to be discovered. Androgenic-anabolic substances tend to reduce triglyceride levels by reducing the concentration of very low density lipoproteins (VLDL): this effect, in itself positive, is inherent in some derivatives of the progestogen nortestosterone, partly the same durabolin, oxandrolone, etc. However, over the past 5 years, they have been found to dramatically lower high-density lipoprotein levels, which carry the “good” portion of cholesterol (that is, HDL, which is the one that clears the arteries), and instead raise cholesterol levels associated with LDL lipoproteins (which Clog the arteries, predisposing to atherosclerosis).
And think that they were even used to treat hypertriglyceridemia! The effect does not depend on the dose, but, by blocking a certain enzymatic pathway, it appears already in small doses, and sometimes within just 2 days. All drugs, regardless of their characteristics (androgenicity, aromatization), seem to share it. Now, this side effect (along with the hypertension, which I will continue about) is the most dangerous mean to me. Not noticing that nothing (while acne and water retention become clearly visible), the arteries become blocked.It cannot be said that atherosclerosis affects all those who take anabolic drugs, but there is no doubt that the risk increases enormously, and not in a probabilistic way ( such as smoking – lung cancer), but much more direct, that is, associated with the duration of… What is usually the first sign of atherosclerosis in a relatively young subject? It is easy to say: death from a heart attack. In the following years, the manifestations, although very serious, become more treatable (with medication, surgery, etc.), but I think you all know what it means to suffer from the heart. Other complications occur at an older age (60-70 years) on the kidneys, brain, etc. Therefore, please do not say that “those who take anabolic are healthy like fish” or something like that: it seems as healthy as a fish, but his arteries are very likely to be destroyed, and would be curious to know if in middle age, especially when you stop exercising, I still feel so good.
Tendency to water retention and hypertension . This side effect is partly dependent on estrogen, but also on the androgen effect itself and / or on the effect on insulin (see above) or endogenous cortisone, all hormones that cause water retention. Water retention in the uninitiated is manifested by edema, especially on the face, ankles; then the bodybuilder, who usually looks in the mirror, will notice the often conspicuous definition, even if the body fat remains the same, that is, it is “smoothed”. Water retention can be roughly measured with a balance: weight that increases rapidly (2-3 days) and disappears just as quickly when the drug is discontinued is nothing more than water retention.Obviously, the most androgenic and flavored foods (testosterone , dianabol, boldenone) are given almost always, even depending on the dose; much less androgenic (methandriol, especially deca) and even less non-aromatized androgens (winstrol, oxandrolone, primobolan)… Of course, it is common knowledge that the ease with which water is retained, even with equal doses of the same drug, varies greatly from person to person, as do all side effects in general: as a rule, people with a tendency to slow metabolism retain more water, probably because Under these conditions, the transformation of steroids is more focused on the production of estrogen (through metabolic 5-beta reduction) than other products (through 5-alpha), and also because the metabolism of cortisol itself is slowed down. Finally, in the same person, the delay is much more apparent with a free diet (carbohydrates) than with a very limited diet. In some cases, retention does not present any other obvious problem besides aesthetic; in others, it is accompanied by an increase in blood pressure. In young and healthy people, the increase in pressure can only be temporary (for several days), because later the mechanisms of self-regulation, as a rule, return it to its place; but in some cases the pressure remains high. Therefore, it is almost imperative that every good gym has a sphygmomanometer, perhaps an automatic type, so that all those who do weight (anabolic or not) can check themselves regularly. Remember that those with very large hands may have falsely higher values of 10-15 mmHg. Art.
Gynecomastia . This means the appearance, to a large extent, of tissue similar to a woman’s breasts in the area behind the nipple. This phenomenon is easily distinguishable from “boobs” in obese males (when the swelling occurs from adipose tissue, and not from the mammary glands), this phenomenon is observed physiologically almost in half of the adolescents, and then disappears. This is naturally due to estrogen. Highly androgenic and aromatized steroids (as well as a diuretic commonly used by bodybuilders, spironolactone or aldactone) can also cause it in adults if taken in excessive doses for extended periods of time… If you allow it to develop, this defect, often even painful, will unfortunately become irreversible (surgery is required).
Liver toxicity . In the past, this has been the most famous side effect of anabolic steroids. In fact, testosterone itself is not toxic to the liver at all, on the contrary, it helps limit the damage it undergoes from numerous toxic substances (alcohol, etc.), so much so that it was once used as an adjuvant in the treatment of liver cirrhosis … The same goes for derivatives. The toxicity attributed to steroids does not depend on the fact that they are steroids, but on the molecular change (alkylation at the 17-alpha position) that many of them have, that is, “traditional” oral. Some injectable drugs are also 17-alpha alkylated (winstrol, methandriol), which is a controversy because alkylation is necessary to prolong the life of orally administered drugs in the body (otherwise the liver will eliminate them immediately). The toxicity of alkylates, as always, depends on time and dose. The first signs consist of inflammation of the bile ducts with jaundice, at first not obvious, and then clinical (the sclera, that is, the white parts of the eyes, are the first areas where jaundice is observed), then an increase in the level of Gamma Gt in the blood. then SGOT and finally SGPT. Many malignant liver tumors (hepatomas) have been attributed to the use of these products, unfortunately, also in bodybuilders.Of course, those who want to check their luggage will say that the tests are not definitive, but in the face of even one similar risk I would say that both it is probably best to avoid taking alkylates that have similar or identical non-toxic liver products.

Finally, another effect of anabolic agents has been attributed to 17-alpha-alkylation, namely the anticoagulant effect… In fact, due to increased fibrinolysis (i.e., the clot is easier to remove), this phenomenon is also observed with non-alkylated products such as ethylestrenol and nandrolones (deca-durabolin). Unless the person has had preexisting coagulation changes, this effect is relatively harmless.
What are the therapeutic indications for these drugs?
Their androgenic characteristics are mainly used to maintain or develop sexual characteristics in cases of deficiency; anabolic performance in case of protein depletion. But let’s see what is mainly used:
- In case of infertility due to azoospermia (i.e. a decrease in sperm count).
- Conditions of low sexual potency (even if due to psychological reasons) can be treated with androgens (typically up to 200 mg / week) given their well-documented role in libido development and maintenance.
- In some cases of breast cancer in women, they are used to curb (unfortunately only palliatively) the development of cancer and pain, in this case, non-aromatized androgens are preferably used in doses that must necessarily be higher than in men: subsequent virilization tolerable given the severity of the disease.
- Anabolic agents have instead been used in cases of protein malnutrition in adults and incorrectly in children (see the case of Dianabol). They improve appetite and, together with proper nutrition, stimulate protein synthesis.
- Similarly, they are used in certain preoperative conditions to improve the trophism of the patient due to severe stress or after the operation itself to facilitate recovery during the recovery period; for the same reason they have been used in severely injured patients or, more generally, in patients forced to lie in bed for extended periods of time to reduce protein catabolism due to stress and / or non-use.
- They are used for severe burns to stimulate faster repair of damaged tissue.
- They are now widely used in the treatment of osteoporosis in both sexes to stimulate bone protein matrix formation and calcium deposition.
- They are often associated with cortisone drugs in chronic therapy to minimize the catabolic effects of these drugs (highly visible on bone, muscle, skin, etc.).
- They are also sometimes used in cases of arthritis or arthrosis and other chronic conditions.
- Finally, for aplastic anemias (that is, those not associated with vitamin B12 or folic acid deficiencies), they were used in very strong doses (before testosterone was used, then we switched to an anabolic drug such as decadurabolin, so as it was seen that the effectiveness was the same, with fewer side effects).
Obviously the average athlete doesn’t get into any of these cases (hopefully); why then do you use anabolic steroids?
Through their use we are trying to stimulate protein synthesis to increase muscle mass and strength, or in resistance to prolonged effort in middle distance athletes. However, the scientific community has not yet been able to demonstrate the effectiveness of these drugs as ergogenic, due in part to the stringency of criteria commonly used in research protocols. Many authors believe that every beneficial effect attributed to steroids is in fact related to the so-called “effect placebo ”(that is, to believe that the substance is good, followed by an improvement in training, etc., in the particular case of the athlete). .
I will cite two of the best studies in this area:
- Fowler et al. in a double-blind study (neither they nor the athletes knew who was taking the placebo or who was taking the drug) tested 47 students aged 28 to 25… 10 were footballers, so athletes trained, the rest were not. Six groups were made (players with half placebos and half drugs, sedentary or not, drug or placebo). Androstenolone was used at a dose of 20 mg per day for 16 weeks. Neither group experienced significant increases in weight, strength, or muscle mass.
- Casner et al conducted a 1971 study on the effect of Winstrol on 27 college students. There were also 4 groups made here: students with placebo or drugs and with or without (resistance) training. Among the parameters measured was a significant increase in body weight in those taking Winstrol, which means that they gained more weight than the placebo. Further analysis, however, appears to make it clear that the weight gain was associated with water retention and not with actual gains in muscle mass. Even here, according to the authors, there was no reason for the use of anabolic steroids in athletes.
HOW TO MINIMIZE SIDE EFFECTS
Unfortunately, those who have decided to take or are already taking anabolic medications will not (I’m afraid) be convinced or intimidated by the above. Although, of course, I do not recommend taking these substances from a medical point of view for the sole purpose of improving athletic performance, of course, many will continue to take them. And therefore it must be said for them that it is also true that, like any other medicine, the frequency of side effects can truly be minimized if the bodybuilder uses steroids correctly. And let’s see how.
Of course, the dose used is a critical factor: let’s explain why with a few small pharmacology notes.
Each drug has the desired action (main effect). At a certain “threshold” dose, nothing happens. Above this dose, the effect manifests itself and increases with increasing dose in an indirect way (i.e…. does not triple when the dose is tripled), but is usually logarithmic. Upon reaching a certain dose, the effect no longer increases, if not insignificantly (property of logarithms), even at doses tens of times higher. Various side effects also have a “range” of reaction, often different from the main effect.
Let’s take testosterone as an example.
Less than 15 mg / week, each effect is minimal. Already at 35 mg / week, a clear nitrogen retention effect is observed. There is no water retention or marked inhibition of gonadotropins at these doses (side effects). By gradually increasing the dose, we will have from 40 to 200 mg per week, first partial and then complete inhibition of gonadotropins. The nitrogen retention effect reaches almost maximum at 200 mg / week, the well-known effect is only twice as high as with a 5-fold reduced dose.
At 400 mg / week, nitrogen retention no longer increases and instead it is clear that water one.
Finally, at doses over 1000 mg (once used to treat certain anemias), virilization and retention are intrusive.
Thus, careful use of a drug that plays at doses already makes a difference.
Another factor related to dose size is the length of the dose period. The discussion is similar to the previous one, Each effect takes its own time.
Water and salt retention is a rather fast process (2-3 days), carbohydrates and potassium are slower, phosphorus is slower (months) and nitrogen is bound to even slower contractile proteins. Inhibition of spermatogenesis is completed in 3-5 months. Then “virilization” (apparently in children and women) occurs very slowly and, as you know, ends in years, not months. The concept of reversibility is also related to duration of action. Virilization is known to be almost irreversible; atherosclerosis is very small if caught early.
It follows from all this that medications, as a rule, should be taken in the shortest possible time necessary for building muscle proteins. Experience shows that a good anabolic effect is achieved after 4-6 weeks: at these doses, testicular atrophy and serum lipid modification are rather scarce.
The concept of dose is perhaps even more important in the case of low androgenic anabolic substances, which, as mentioned at the beginning are usually true at low doses. and they become more androgenic at higher doses. Using steroids that are too high and causing more side effects will only increase your risk of becoming “insensitive” to the drug itself. This phenomenon, typical of endocrinology, may be due to the fact that the cellular structures responsible for recognizing steroids and receiving the message of war (receptors) decrease in number if they are exposed for a long time to too high concentrations of the same, as to protect cells from overdose.
This phenomenon is called down-regulation (sub-regulation) and is also typical of thyroid hormones (beware !!!), insulin and other hormones ..
Well, many so-called drug formulators believe that switching from one steroid to another is a method of eliminating downregulation.
You won’t believe that mother nature has created as many different types of receptors as there are steroids. on the market! There is only one steroid receptor, and if it decreases, the effect of any anabolic steroid will decrease. It also follows how wrong another typical bodybuilding practice is: stacking (using two or more steroids together) or even “bombarding” (megadoses of different drugs, type 100 deca, 200 testosterone, 200 primobolan … per day!): If the receptor ( poor guy) only one, you only put it in your underwear.
Rather, it must be said that just because the receptor is the same does not mean that different foods have the same effect. In fact, once inside the cell, the steroid can be metabolized in different ways (I mentioned this earlier), causing different effects: c. for example, a more noticeable increase in phosphocreatine and mitochondria for a more androgenic (“massive” effect), a more noticeable increase in contractile proteins for a less androgenic (“power” effect), etc.
I advise you to re-read well what I wrote and keep this in mind. During steroid therapy (and even after its termination) it would be good to check at least the following indicators:
- pressure once a week
- Body weight every day (an increase of more than 1 kg per week is an undeniable indicator of water retention)
- A in the blood – SGOT, SGPT, Gamma-Gt, bilirubins, total cholesterol, triglycerides and HDL cholesterol (or protein electrophoresis).
- Every 3-6 months, especially if you are under strong androgen, you should have a rectal exam.
It is not advisable to bring these tests to your doctor, unless he is an expert in the field and is not friendly with you, Seek a doctor who knows the environment and whom you trust to help you interpret the tests in light the fact that you are taking steroids.
If, at last, side effects appear, what to do? I have to say this on an individual basis. However, in general I would say:
- If liver enzymes (SGOT, SGPT, Gamma-Gt or Bilirubin) change, stop using 17-alpha alkylates (Winstrol, Oxandrolon abnehmen, Dianabol, etc.) and forget about them for the rest of your life. If you didn’t take them instead, it’s very likely that you have real liver disease, regardless of steroids..
- If you have a tendency to have low HDL cholesterol levels even in normal conditions and / or family members (dad, uncle, grandparents) with a history of heart attack, check this index very carefully and, if you really need to, do short cycles. Then try (but that’s even if you’re not on steroids) regularly aerobics throughout your life (that’s not what I’m talking about in terms of sports prevention, I’m not talking here).
- In case of acne, avoid ignoring it until you become a leper. Miracles don’t work here, just: a) avoid using highly androgenic products and do not exceed therapeutic doses b) cleanse your skin properly and use antibiotic ointments (although acne, although androgens prefer them, is a bacterial infection) c) try to stay in the sun if it is possible.
- In the case of gynecomastia, you will almost always find testosterone or dianabol responsible. Well, all you have to do is stop them and you won’t have to take any more flavored drugs.
- In the event of excessive (for your usual purposes) water retention, reduce the doses and you will see this phenomenon almost always subside. If this continues, be aware that there are other ways to reduce water retention, many of which are possibly worse than water retention ..
One more article is required for their exhaustive consideration, so I will only mention:
- Diuretics : they deplete salts, the effect is often uncontrollable, and if you really need to, use them for several days (and with appropriate supplementation) of minerals, which is strictly dependent on the diuretic or combinations of diuretics used). They can be very dangerous (if not for life, of course for a sports presentation: consider doing weight or doing cramps racing …)… However, diuretics were recently banned from IFBB racing.
- Antiestrogens : (tamoxifen or nolvadex, testonolactone and testolac, cyclophenyl). They are quite toxic drugs in the long run; they tend to give a slurry rebound effect (that is, when you stop them, you swell like balls), and this only acts on the estrogenic component of water retention anyway. Better not to use them at all. Their use can only be reserved for those who (often, even if they do not take anything) have really high estrogen levels (above 40 pg / ml, as confirmed by a blood test that still takes it) and suffer from delay
- Diet Monitoring . Of course, if you limit the amount of carbohydrates, the delay disappears, but it doesn’t make sense if you are in the mass phase. Better to limit your sodium intake with a computerized diet: I say, limit, don’t rule out, because if you eat too little you will lose potassium, and even then you will have a blessed rebound (due to overproduction of the sodium-friendly hormone aldosterone ) and you would be very bloated like frogs if you eat food rich in salt. Instead of salt, limiting water intake, which is more than dangerous, is completely useless (the body sets up systems to retain even the small amount that you must take).
Finally, among natural systems, the most effective and beneficial is undoubtedly the regular practice of aerobic activities, such as running or cycling, which, unfortunately, almost no one does. Those who tend to suffer from retention should gradually engage in aerobics (not dance!) And stay in training… It is not true that running makes you lose muscle; it only does so if, due to too low aerobic fitness (where you are, of course, if you are doing weights only), you increase your running doses too quickly.
And the last, the last word for women: I leave aside the debate about whether women should be muscular or rather flexible and slim (soft, tough, etc.). From a purely medical point of view, a woman who really wants to take an anabolic should definitely do it under the strict supervision of a specialist doctor (endocrinologist), since ultimately these are male hormones. In addition to the side effects associated with more or less pronounced masculinization, there is a risk of damage to all female functions (menstruation, possibility of pregnancy) due to their very delicate nature.
Read more about this article
I liked this article primarily because it focuses on aspects of AAS danger that are usually ignored: we usually only deal with the axis, pituitary, gynuids and liver. But no one has ever died of hypogonadism, and even cases of liver tumors are indeed rare and statistically insignificant. Instead, it’s clear that premature deaths from heart attacks are more common in bodybuilders…. The fact that bomber jackets are the least affected by cancer in the US population does not permit myocardial suicide.However, to make prevention as effective as possible, it is good to be as precise as possible, so two more words on how negative is expressed. the effect of AAS on lipids; is an effect that, in addition to being dose dependent, is formulated differently according to certain characteristics of the AAS:
- alkylates show the ability to worsen the HDL / LDL ratio at any dosage, even if they sometimes lower total cholesterol (especially oxandrolone and furazabol);
- unalkylated, on the other hand, exhibit this effect only at various high doses, depending on the specific substance, with non-flavorants, which exhibit this attitude at lower doses than with flavored; even fragrances have the paradoxical effect of improving lipids at the lowest doses.
For example, testosterone enanthate at a dose of 100 mg per week shows a clear lipid-enhancing effect, which, although decreasing, still remains at 300 mg; at 600 mg it leaves them unchanged, and at 900 the negative effect is evident. Probably, in men suffering from hypogonadism, this data will have to be slightly retouched upwards. For the prostate, I would be less alarmist: it is now established that benign hypertrophy is caused by estrogens and progestins, while for malignant there is no evidence of a connection with androgens: the experiment that started this dogma was from 1941 and is completely unreliable for the methods of execution and also for the partial report to which he was subject. For women, the discussion goes against the usual discussion in men of not only fertility loss, which is sometimes welcome, but also the specific dependence of female hormones, as well as the positive effects that AAS can have…. in counteracting those psycho-nutritional disorders that women are more likely to experience
Let’s pause for a moment to think about the side effects, which are arguably the worst of the short term. As for the sexual ones, you think they are an advantage.
We say yes, but I must remember that an increase in libido, if not satisfied (Freud teaches …), can transform into other types of drives, up to before the crime. Finally, remember that an initial increase inevitably follows a decrease after suspension for the physiological reasons explained above. When it comes to the impact on aggression, I remember that they often wish bodybuilders or powerlifters to go to the gym more busy to lift huge weights. I do not deny that it is effective, but at what cost! If you really feel like you need the extra nerve to gain weight, it can mean many things, for example:
- You are probably mildly overtrained or the routine is boring and unproductive;
- You have other psychological problems;
- You are not made for this sport;
- In all the above cases, you are still wrong.
Dealing with these anabolic psychological “disorders” is absurd; It is better to act at the root of the problem, eliminate harmful causes and learn to control your mind, how to control your muscles. There are special methods for all this (self-hypnosis, autogenous training). As for other anabolic steroids, it should be said that their effect on libido and aggression seems to be related to the degree of androgenicity: from my own experience, I have even seen that few androgenic products (such as winstrol) in some subjects there is a tendency to decrease even libido if used alone: however, this should not be dependent on a decrease in gonadotropins.
Now let’s look at some other effects, not necessarily related to the androgenicity of foods. These include:
- Altered blood sugar . Androgenic anabolic agents can increase insulin sensitivity, this usually does not lead to hypoglycemia, but to a possible increase in its effects, that is, increase in fat, water retention, etc. These phenomena seem to be more pronounced in drugs that are sensitive to peripheral aromatization.
- Modification of blood lipids (fats) . I will dwell on this aspect for a moment, among the latter to be discovered. Androgenic-anabolic substances tend to reduce triglyceride levels by reducing the concentration of very low density lipoproteins (VLDL): this effect, in itself positive, is inherent in some derivatives of the progestogen nortestosterone, partly the same durabolin, oxandrolone, etc. However, over the past 5 years, they have been found to dramatically lower high-density lipoprotein levels, which carry the “good” portion of cholesterol (that is, HDL, which is the one that clears the arteries), and instead raise cholesterol levels associated with LDL lipoproteins (which “Pollute” the arteries, causing a predisposition to atherosclerosis). And think that they were even used to treat hypertriglyceridemia! The effect does not depend on the dose, but, by blocking a certain enzymatic pathway, it appears already in small doses, and sometimes within just 2 days. All drugs, regardless of their characteristics (androgenicity, aromatization), seem to share it. Now, this side effect (along with the hypertension, which I will continue about) is for me the most dangerous vile… Without noticing that nothing (while acne and water retention become clearly visible), the arteries become blocked, It cannot be said that atherosclerosis affects all those who take anabolic drugs, but it is undoubted that the risk increases enormously, and not in a probabilistic way ( such as smoking – lung cancer), but much more direct, that is, associated with the duration of intake. What is usually the first sign of atherosclerosis in a relatively young subject? It is easy to say: death from a heart attack. In the following years, the manifestations, although very serious, become more treatable (with medication, surgery, etc.), but I think you all know what it means to suffer from the heart. Other complications occur at an older age (60-70 years) on the kidneys, brain, etc. Therefore, please do not say that “those who take anabolic are healthy as fish” or something like that: it seems healthy as a fish, but his arteries are very likely to be destroyed, and would be curious to know if middle age, especially when you stop exercising, still feel so good.
- Tendency to water retention and hypertension . This side effect is partly dependent on estrogen, but also on the androgen effect itself and / or on the effect on insulin (see above) or endogenous cortisone, all hormones that cause water retention. Water retention in the uninitiated is manifested by edema, especially on the face, ankles; then the bodybuilder, who usually looks in the mirror, will notice the often conspicuous definition, even if the body fat remains the same, that is, it is “smoothed”… Water retention can be roughly measured with a balance: weight that increases rapidly (2-3 days) and disappears just as quickly when the drug is discontinued is nothing more than water retention.Obviously, the most androgenic and flavored foods (testosterone , dianabol, boldenone) are given almost always, even depending on the dose; much less small androgens (methandriol, especially deca) and even less small non-aromatized androgens (winstrol, oxandrolone, primobolan). Of course, it is common knowledge that the ease with which water is retained, even with equal doses of the same drug, varies greatly from person to person, as do all side effects in general: as a rule, people with a tendency to slow metabolism retain more water, probably because Under these conditions, the transformation of steroids is more focused on the production of estrogen (through metabolic 5-beta reduction) than other products (through 5-alpha), and also because the metabolism of cortisol itself is slowed down. Finally, in the same person, the delay is much more apparent with a free diet (carbohydrates) than with a very limited diet. In some cases, retention does not present any other obvious problem besides aesthetic; in others, it is accompanied by an increase in blood pressure. In young and healthy people, the increase in pressure can only be temporary (for several days), because later the mechanisms of self-regulation, as a rule, return it to its place; but in some cases the pressure remains high. Therefore, it is almost imperative that every good gym has a sphygmomanometer, perhaps an automatic type, so that all those who do weight (anabolic or not) can check themselves regularly. Remember that those with very large hands may have falsely higher values of 10-15 mm / Hg. Art.
- gynecomastia … This means the appearance, to a large extent, of tissue similar to a woman’s breasts in the area behind the nipple. This phenomenon is easily distinguishable from “boobs” in obese males (when the swelling occurs from adipose tissue, and not from the mammary glands), this phenomenon is observed physiologically almost in half of the adolescents, and then disappears. This is naturally due to estrogen. Highly androgenic and aromatized steroids (as well as a diuretic commonly used by bodybuilders, spironolactone or aldactone) can also cause it in adults if taken in excessive doses for extended periods of time. If you allow it to develop, this defect, often even painful, unfortunately, will become irreversible (surgery is required).
- Liver toxicity . In the past, this has been the most famous side effect of anabolic steroids. In fact, testosterone itself is not toxic to the liver at all, on the contrary, it helps limit the damage it undergoes from numerous toxic substances (alcohol, etc.), so much so that it was once used as an adjuvant in the treatment of liver cirrhosis … The same goes for derivatives. The toxicity attributed to steroids does not depend on the fact that they are steroids, but on the molecular change (alkylation at the 17-alpha position) that many of them have, that is, “traditional” oral. Some injectable drugs are also 17-alpha alkylated (winstrol, methandriol), which is a controversy because alkylation is necessary to prolong the life of orally administered drugs in the body (otherwise the liver will eliminate them immediately). The toxicity of alkylates, as always, depends on time and dose. The first signs consist of inflammation of the bile ducts with jaundice, at first not obvious, and then clinical (the sclera, that is, the white parts of the eyes, are the first areas where jaundice is observed), then an increase in the level of Gamma Gt in the blood. then SGOT and finally SGPT… Many malignant liver tumors (hepatomas) have been attributed to the use of these products, unfortunately, also in bodybuilders.Of course, those who want to check their luggage will say that the tests are not definitive, but in the face of even such a risk I would say that how can rather, it is best to avoid taking alkylates that have similar or identical non-toxic liver products.
Finally, another effect of anabolic agents has been attributed to 17-alpha-alkylation, namely the anticoagulant effect. In fact, due to increased fibrinolysis (i.e., the clot is easier to remove), this phenomenon is also observed with non-alkylated products such as ethylestrenol and nandrolones (deca-durabolin). Unless the person has had any pre-existing coagulation changes, this effect is relatively harmless.
What are the therapeutic indications for these drugs?
Their androgenic characteristics are mainly used to maintain or develop sexual characteristics in cases of deficiency; anabolic performance in case of protein depletion. But let’s see what is mainly used:
- In case of infertility due to azoospermia (i.e. a decrease in sperm count).
- Conditions of low sexual potency (even if due to psychological reasons) can be treated with androgens (usually up to 200 mg / week) given their well-documented role in the development and maintenance of libido.
- In some cases of breast cancer in women, they are used to curb (unfortunately only palliatively) the development of cancer and pain, in this case, non-aromatized androgens are preferably used in doses that must necessarily be higher than in men: subsequent virilization tolerable given the severity of the disease.
- Anabolic agents have instead been used in cases of protein malnutrition in adults and incorrectly in children (see… the case of Dianabol), They improve appetite and, together with proper nutrition, stimulate protein synthesis.
- Similarly, they are used in certain preoperative conditions to improve the trophism of the patient due to severe stress or after the operation itself to facilitate recovery during the recovery period; for the same reason they have been used in severely injured patients or more generally in patients who have to lie in bed for extended periods of time to reduce protein catabolism due to stress and / or disuse.
- They are used for severe burns to stimulate faster repair of damaged tissue.
- They are now widely used in the treatment of osteoporosis in both sexes to stimulate bone protein matrix formation and calcium deposition.
- They are often associated with cortisone drugs in chronic therapy to minimize the catabolic effects of these drugs (highly visible on bone, muscle, skin, etc.).
- They are also sometimes used in cases of arthritis or arthrosis and other chronic conditions.
- Finally, for aplastic anemias (that is, those not associated with vitamin B12 or folic acid deficiencies), they were used in very strong doses (before testosterone was used, then we switched to an anabolic drug such as decadurabolin, so as it was seen that the effectiveness was the same, with fewer side effects).
Obviously the average athlete doesn’t get into any of these cases (hopefully); why then do you use anabolic steroids?
Through their use we are trying to stimulate protein synthesis to increase muscle mass and strength, or resistance to prolonged effort in middle distance athletes… However, the scientific community has not yet been able to demonstrate the effectiveness of these drugs as ergogenic, due in part to the stringency of criteria commonly used in research protocols. Many authors believe that every beneficial effect attributed to steroids is in fact related to the so-called “effect placebo ”(that is, to believe that the substance is good, followed by an improvement in training, etc., in the particular case of the athlete). .
I will cite two of the best studies in this area:
- Fowler et al. in a double-blind study (neither they nor the athletes knew who was taking the placebo or who was taking the drug) tested 47 students between the ages of 28 and 25. 10 were footballers, so athletes trained, the rest were not. Six groups were made (players with half placebos and half drugs, sedentary or not, drug or placebo). Androstenolone was used at a dose of 20 mg per day for 16 weeks. Neither group experienced significant increases in weight, strength, or muscle mass.
- Casner et al conducted a 1971 study on the effect of Winstrol on 27 college students. There were also 4 groups made here: students with placebo or drugs and with or without (resistance) training. Among the parameters measured was a significant increase in body weight in those taking Winstrol, which means that they gained more weight than the placebo. Further analysis, however, appears to make it clear that the weight gain was associated with water retention and not with actual gains in muscle mass. Even here, according to the authors, there was no reason for the use of anabolic steroids in athletes.
HOW TO MINIMIZE SIDE EFFECTS
Unfortunately, those who have decided to take or are already taking anabolic medications will not (I am afraid) be convinced or afraid of the above… Although, of course, I do not recommend taking these substances from a medical point of view for the sole purpose of improving athletic performance, of course, many will continue to take them. And therefore it must be said for them that it is also true that, like any other medicine, the frequency of side effects can truly be minimized if the bodybuilder uses steroids correctly. And let’s see how.
Of course, the dose used is a critical factor: let’s explain why with a few small pharmacology notes.
Each drug has the desired action (main effect). At a certain “threshold” dose, nothing happens. Above this dose, the effect manifests itself and increases with increasing dose indirectly (i.e., it does not triple when the dose is threefold), but is usually logarithmic. Upon reaching a certain dose, the effect no longer increases, if not insignificantly (property of logarithms), even at doses tens of times higher. Various side effects also have a “range” of reaction, often different from the main effect.
Let’s take testosterone as an example.
Less than 15 mg / week, each effect is minimal. Already at 35 mg / week, a clear nitrogen retention effect is observed. There is no water retention or marked inhibition of gonadotropins at these doses (side effects). By gradually increasing the dose, we will have from 40 to 200 mg per week, first partial and then complete inhibition of gonadotropins. The nitrogen retention effect reaches almost maximum at 200 mg / week, the well-known effect is only twice as high as with a 5-fold reduced dose.
At 400 mg / week, nitrogen retention no longer increases and instead it is clear that water one.
Finally, in doses greater than 1000 mg (once used to treat some anemias), virilization and retention is imposed. difference.
Another factor related to dose size is the length of the dose period… The discussion is similar to the previous one, Each effect takes its own time.
Water and salt retention is a rather fast process (2-3 days), carbohydrates and potassium are slower, phosphorus is slower (months) and nitrogen is bound to even slower contractile proteins. Inhibition of spermatogenesis is completed in 3-5 months. Then “virilization” (apparently in children and women) occurs very slowly and, as you know, ends in years, not months. The concept of reversibility is also related to duration of action. Virilization is known to be almost irreversible; atherosclerosis is very small if caught early.
It follows from all this that medications, as a rule, should be taken in the shortest possible time necessary for building muscle proteins. Experience shows that a good anabolic effect is achieved after 4-6 weeks: at these doses, testicular atrophy and serum lipid modification are rather scarce.
The concept of dose is perhaps even more important in the case of low androgenic anabolic substances, which, as mentioned at the beginning are usually true at low doses. and they become more androgenic at higher doses. Using steroids that are too high and causing more side effects will only increase your risk of becoming “insensitive” to the drug itself. This phenomenon, typical of endocrinology, may be due to the fact that the cellular structures responsible for recognizing steroids and receiving the message of war (receptors) decrease in quantity if they are exposed for a long time to too high concentrations of the same, as to protect the cell from overdose.
This phenomenon is called down-regulation (sub-regulation) and is also typical of thyroid hormones (beware !!!), insulin and other hormones ..
Well, many so-called formulators believe that switching from one steroid to another is a method of eliminating downregulation.
You won’t believe that mother nature has created as many different types of receptors as steroids. on the market! There is only one steroid receptor, and if it decreases, the effect of any anabolic steroid will decrease. It also follows how wrong another typical bodybuilding practice is: stacking (using two or more steroids together) or even “bombarding” (megadoses of different drugs, type 100 deca, 200 testosterone, 200 primobolan … per day!): If the receptor ( poor fellow) only one, you put it only in your underwear.
Rather, it must be said that if the receptor is the same, this does not mean that different products have the same effect. In fact, once inside the cell, the steroid can be metabolized in different ways (I mentioned this earlier), causing different effects: c. for example, a more noticeable increase in phosphocreatine and mitochondria for a more androgenic (“massive” effect), a more noticeable increase in contractile proteins for a less androgenic (“power” effect), etc.
I advise you to re-read well what I wrote and keep this in mind. During steroid therapy (and even after its termination) it would be good to check at least the following indicators:
- pressure once a week
- Body weight every day (an increase of more than 1 kg per week is an undeniable indicator of water retention)
- A in the blood – SGOT, SGPT, Gamma-Gt, bilirubins, total cholesterol, triglycerides and HDL cholesterol (or protein electrophoresis).
- Every 3-6 months, especially if you are under strong androgen, you should have a rectal exam.
It is not advisable to bring these tests to your doctor, unless he is an expert in the field and is not friendly with you, Seek a doctor who knows the environment and whom you trust to help you interpret the tests in light the fact that you are taking steroids.
If, at last, side effects appear, what to do? I have to say this on an individual basis. However, in general I would say:
- If liver enzymes (SGOT, SGPT, Gamma-Gt or Bilirubin) change, stop using 17-alpha alkylates (Winstrol, Oxandrolone, Dianabol, etc.) and forget about them for the rest of your life. If you didn’t take them instead, it’s very likely that you have real liver disease, regardless of steroids.
- If you have a tendency to have low HDL cholesterol levels even in normal conditions and / or family members (dad, uncle, grandparents) with a history of heart attack, check this index very carefully and, if you really need to, do short cycles. Then try (but that’s even if you’re not on steroids) regularly aerobics throughout your life (that’s not what I’m talking about in terms of sports prevention, I’m not talking here).
- In the event of acne, avoid ignoring it until you become a leper. Miracles don’t work here, just: a) avoid using highly androgenic products and do not exceed therapeutic doses b) cleanse your skin properly and use antibiotic ointments (although acne, although androgens prefer them, is a bacterial infection) c) try to stay in the sun if it is possible.
- In the case of gynecomastia, you will almost always find testosterone or dianabol responsible. Well, all you can do is stop them and you won’t have to take any more flavored drugs.
- In the event of excessive (for your usual purposes) water retention, reduce the doses and you will see this phenomenon almost always subside. If this continues, be aware that there are other ways to reduce water retention, many of which are arguably worse than having it..
One more article is required for their exhaustive consideration, so I will only mention:
- Diuretics : they deplete salts, the effect is often uncontrollable, and if you really need to, use them for several days (and with appropriate supplementation) of minerals, which is strictly dependent on the diuretic or combinations of diuretics used). They can be very dangerous (if not for life, of course, for a sports presentation: consider doing weight or doing cramps racing …). However, diuretics were recently banned from IFBB racing.
- Antiestrogens : (tamoxifen or nolvadex, testonolactone and testolac, cyclophenyl). They are quite toxic drugs in the long run; they tend to give a slurry rebound effect (that is, when you stop them, you swell like balls), and this only acts on the estrogenic component of water retention anyway. Better not to use them at all. Their use can only be reserved for those who (often, even if they do not take anything) have really high estrogen levels (above 40 pg / ml, as confirmed by a blood test that still takes it) and suffer from delay
- Diet Monitoring . Of course, if you limit the amount of carbohydrates, the delay disappears, but it doesn’t make sense if you are in the mass phase. Better to limit your sodium intake with a computerized diet: I say, limit, don’t rule out, because if you eat too little you will lose potassium, and even then you will have a blessed rebound (due to overproduction of the sodium-friendly hormone aldosterone ) and you would be very bloated like frogs if you eat food rich in salt… Instead of salt, limiting water intake, which is more than dangerous, is completely useless (the body sets up systems to retain even the small amount that you must take).
Finally, among natural systems, the most effective and beneficial is undoubtedly the regular practice of aerobic activities, such as running or cycling, which, unfortunately, almost no one does. Those who tend to suffer from retention should gradually practice aerobics (not dance!) And stay in training. It is not true that running makes you lose muscle; it only does so if, due to too low aerobic fitness (where you are, of course, if you are doing weights only), you increase your running doses too quickly.
And the last, the last word for women: I leave aside the debate about whether women should be muscular or rather flexible and slim (soft, tough, etc.). From a purely medical point of view, a woman who really wants to take an anabolic should definitely do it under the strict supervision of a specialist doctor (endocrinologist), since ultimately these are male hormones. In addition to the side effects associated with more or less pronounced masculinization, there is a risk of damage to all female functions (menstruation, possibility of pregnancy) due to their very delicate nature.
Gynecomastia. This means the appearance, to a large extent, of tissue similar to a woman’s breasts in the area behind the nipple. This phenomenon is easily distinguishable from “boobs” in obese males (when the swelling occurs from adipose tissue, and not from the mammary glands), this phenomenon is observed physiologically almost in half of the adolescents, and then disappears. This is naturally due to estrogen. Highly androgenic and aromatized steroids (as well as a diuretic commonly used by bodybuilders, spironolactone or aldactone) can also cause it in adults if taken in excessive doses for extended periods of time. If you allow it to develop, this defect, often even painful, will unfortunately become irreversible (surgery is required).
Liver toxicity. In the past, this has been the most famous side effect of anabolic steroids. In fact, testosterone itself is not toxic to the liver at all, on the contrary, it helps limit the damage it undergoes from numerous toxic substances (alcohol, etc.), so much so that it was once used as an adjuvant in the treatment of liver cirrhosis … The same goes for derivatives. The toxicity attributed to steroids does not depend on the fact that they are steroids, but on the molecular change (alkylation at the 17-alpha position) that many of them have, that is, “traditional” oral. Some injectable drugs are also 17-alpha alkylated (winstrol, methandriol), which is a controversy because alkylation is necessary to prolong the life of orally administered drugs in the body (otherwise the liver will eliminate them immediately). The toxicity of alkylates, as always, depends on time and dose. The first signs consist of inflammation of the bile ducts with jaundice, at first not obvious, and then clinical (the sclera, that is, the white parts of the eyes, are the first areas where jaundice is observed), then an increase in the level of Gamma Gt in the blood. then SGOT and finally SGPT. Many malignant liver tumors (hepatomas) have been attributed to the use of these products, unfortunately, also in bodybuilders.Of course, those who want to check their luggage will say that the tests are not definitive, but in the face of even one similar risk I would say that both it is probably best to avoid taking alkylates that have similar or identical non-toxic liver products.
Finally, another effect of anabolic agents has been attributed to 17-alpha-alkylation, namely the anticoagulant effect. In fact, due to increased fibrinolysis (i.e., the clot is easier to remove), this phenomenon is also observed with non-alkylated products such as ethylestrenol and nandrolones (deca-durabolin). Unless the person has had preexisting coagulation changes, this effect is relatively harmless.
What are the therapeutic indications for these drugs?
Their androgenic characteristics are mainly used to maintain or develop sexual characteristics in cases of deficiency; anabolic performance in case of protein depletion. But let’s see what is mainly used:
- In case of infertility due to azoospermia (i.e. a decrease in sperm count).
- Conditions of low sexual potency (even if due to psychological reasons) can be treated with androgens (typically up to 200 mg / week) given their well-documented role in libido development and maintenance.
- In some cases of breast cancer in women, they are used to curb (unfortunately only palliatively) the development of cancer and pain, in this case, non-aromatized androgens are preferably used in doses that must necessarily be higher than in men: subsequent virilization tolerable given the severity of the disease.
- Anabolic agents have instead been used in cases of protein malnutrition in adults and incorrectly in children (see the case of Dianabol). They improve appetite and, together with proper nutrition, stimulate protein synthesis.
- Similarly, they are used in certain preoperative conditions to improve the trophism of the patient due to severe stress or after the operation itself to facilitate recovery during the recovery period; for the same reason they have been used in severely injured patients or more generally in patients who have to lie in bed for extended periods of time to reduce protein catabolism due to stress and / or disuse.
- They are used for severe burns to stimulate faster repair of damaged tissue.
- They are now widely used in the treatment of osteoporosis in both sexes to stimulate bone protein matrix formation and calcium deposition.
- They are often associated with cortisone drugs in chronic therapy to minimize the catabolic effects of these drugs (highly visible on bone, muscle, skin, etc.).
- They are also sometimes used in cases of arthritis or arthrosis and other chronic conditions.
- Finally, for aplastic anemias (that is, those not associated with vitamin B12 or folic acid deficiencies), they were used in very strong doses (before testosterone was used, then we switched to an anabolic drug such as decadurabolin, so as it was seen that the effectiveness was the same, with fewer side effects).
Obviously the average athlete doesn’t get into any of these cases (hopefully); why then do you use anabolics?
Through their use, we are trying to stimulate protein synthesis to increase muscle mass and strength, or resistance to sustained effort in mid-distance athletes. However, the scientific community has not yet been able to demonstrate the effectiveness of these drugs as ergogenic, due in part to the stringency of criteria commonly used in research protocols. Many authors believe that every beneficial effect attributed to steroids is in fact related to the so-called “effect placebo ”(that is, to believe that the substance is good, followed by an improvement in training, etc., in the particular case of the athlete). .
I will cite two of the best studies in this area:
- Fowler et al. in a double-blind study (neither they nor the athletes knew who was taking the placebo or who was taking the drug) tested 47 students between the ages of 28 and 25. 10 were footballers, so athletes trained, the rest were not. Six groups were made (players with half placebos and half drugs, sedentary or not, drug or placebo). Androstenolone was used at a dose of 20 mg per day for 16 weeks. Neither group experienced significant increases in weight, strength, or muscle mass.
- Casner et al conducted a 1971 study on the effect of Winstrol on 27 college students. There were also 4 groups made here: students with placebo or drugs and with or without (resistance) training. Among the parameters measured was a significant increase in body weight in those taking Winstrol, which means that they gained more weight than the placebo. Further analysis, however, appears to make it clear that the weight gain was associated with water retention and not with actual gains in muscle mass. Even here, according to the authors, there was no reason for the use of anabolic steroids in athletes.
HOW TO MINIMIZE SIDE EFFECTS
Unfortunately, those who have decided to take or are already taking anabolic drugs will not (I fear) be convinced or intimidated by the above. Although, of course, I do not recommend taking these substances from a medical point of view for the sole purpose of improving athletic performance, of course, many will continue to take them. And therefore it must be said for them that it is also true that, like any other medicine, the frequency of side effects can truly be minimized if the bodybuilder uses steroids correctly. And let’s see how.
Of course, the dose used is a critical factor: let’s explain why with a few small pharmacology notes.
Each drug has the desired action (main effect). At a certain “threshold” dose, nothing happens. Above this dose, the effect manifests itself and increases with increasing dose indirectly (i.e., it does not triple when the dose is threefold), but is usually logarithmic. Upon reaching a certain dose, the effect no longer increases, if not insignificantly (property of logarithms), even at doses tens of times higher. Various side effects also have a “range” of reaction, often different from the main effect.
Let’s take testosterone as an example.
Less than 15 mg / week, each effect is minimal. Already at 35 mg / week, a clear nitrogen retention effect is observed. There is no water retention or marked inhibition of gonadotropins at these doses (side effects). By gradually increasing the dose, we will have from 40 to 200 mg per week, first partial and then complete inhibition of gonadotropins. The nitrogen retention effect reaches almost maximum at 200 mg / week, the well-known effect is only twice as high as with a 5-fold reduced dose.
At 400 mg / week, nitrogen retention no longer increases and instead it is clear that water one.
Finally, at doses over 1000 mg (once used to treat certain anemias), virilization and retention are intrusive.
Thus, careful use of a drug that plays at doses already makes a difference.
Another factor related to dose size is the length of the dose period. The discussion is similar to the previous one, Each effect takes its own time.
Water and salt retention is a rather fast process (2-3 days), carbohydrates and potassium are slower, phosphorus is slower (months) and nitrogen is bound to even slower contractile proteins. Inhibition of spermatogenesis is completed in 3-5 months. Then “virilization” (apparently in children and women) occurs very slowly and, as you know, ends in years, not months. The concept of reversibility is also related to duration of action. Virilization is known to be almost irreversible; atherosclerosis is very small if caught early.
It follows from all this that medications, as a rule, should be taken in the shortest possible time necessary for building muscle proteins. Experience shows that a good anabolic effect is achieved after 4-6 weeks: at these doses, testicular atrophy and serum lipid modification are rather scarce.
The concept of dose is perhaps even more important in the case of low androgenic anabolic substances, which, as mentioned at the beginning, are usually true at low doses. and they become more androgenic at higher doses. Using steroids that are too high and causing more side effects will only increase your risk of becoming “insensitive” to the drug itself. This phenomenon, typical of endocrinology, may be due to the fact that the cellular structures responsible for recognizing steroids and receiving the message of war (receptors) decrease in number if they are exposed for a long time to too high concentrations of the same, as to protect cells from overdose.
This phenomenon is called down-regulation (sub-regulation) and is also typical of thyroid hormones (beware !!!), insulin and other hormones ..
Well, many so-called drug formulators believe that switching from one steroid to another is a method of eliminating downregulation.
You won’t believe that mother nature has created as many different types of receptors as there are steroids. on the market! There is only one steroid receptor, and if it decreases, the effect of any anabolic steroid will decrease. It also follows how wrong another typical bodybuilding practice is: stacking (using two or more steroids together) or even “bombarding” (megadoses of different drugs, type 100 deca, 200 testosterone, 200 primobolan … per day!): If the receptor ( poor guy) only one, you only put it in your underwear.
Rather, it must be said that just because the receptor is the same does not mean that different foods have the same effect. In fact, once inside the cell, the steroid can be metabolized in different ways (I mentioned this earlier), causing different effects: c. for example, a more noticeable increase in phosphocreatine and mitochondria for a more androgenic (“massive” effect), a more noticeable increase in contractile proteins for a less androgenic (“power” effect), etc.
I advise you to re-read well what I wrote and keep this in mind. During steroid therapy (and even after its termination) it would be good to check at least the following indicators:
- pressure once a week
- Body weight every day (an increase of more than 1 kg per week is an undeniable indicator of water retention)
- A in the blood – SGOT, SGPT, Gamma-Gt, bilirubins, total cholesterol, triglycerides and HDL cholesterol (or protein electrophoresis).
- Every 3-6 months, especially if you are under strong androgen, you should have a rectal exam.
It is not advisable to bring these tests to your doctor, unless he is an expert in the field and is not friendly with you, Seek a doctor who knows the environment and whom you trust to help you interpret the tests in light the fact that you are taking steroids.
If, at last, side effects appear, what to do? I have to say this on an individual basis. However, in general I would say:
- If liver enzymes (SGOT, SGPT, Gamma-Gt or Bilirubin) change, stop using 17-alpha alkylates (Winstrol, Oxandrolone, Dianabol, etc.) and forget about them for the rest of your life. If you didn’t take them instead, it’s very likely that you have real liver disease, regardless of steroids.
- If you have a tendency to have low HDL cholesterol levels even in normal conditions and / or family members (dad, uncle, grandparents) with a history of heart attack, check this index very carefully and, if you really need to, do short cycles. Then try (but that’s even if you’re not on steroids) regularly aerobics throughout your life (that’s not what I’m talking about in terms of sports prevention, I’m not talking here).
- In case of acne, avoid ignoring it until you become a leper. Miracles don’t work here, just: a) avoid using highly androgenic products and do not exceed therapeutic doses b) cleanse your skin properly and use antibiotic ointments (although acne, although androgens prefer them, is a bacterial infection) c) try to stay in the sun if it is possible.
- In the case of gynecomastia, you will almost always find testosterone or dianabol responsible. Well, all you have to do is stop them and you won’t have to take any more flavored drugs.
- In the event of excessive (for your usual purposes) water retention, reduce the doses and you will see this phenomenon almost always subside. If this continues, be aware that there are other ways to reduce water retention, many of which are possibly worse than water retention ..
One more article is required for their exhaustive consideration, so I will only mention:
- Diuretics: they deplete salts, the effect is often uncontrollable, and if you really need to use them for a few days (and with the appropriate supplementation) of minerals, which strictly depends on the diuretic or the combination of diuretics used). They can be very dangerous (if not for life, of course, for a sports presentation: consider doing weight or doing cramps racing …). However, diuretics were recently banned from IFBB racing.
- Antiestrogens : (tamoxifen or nolvadex, testonolactone and testolac, cyclophenyl). They are quite toxic drugs in the long run; they tend to give a slurry rebound effect (that is, when you stop them, you swell like balls), and this only acts on the estrogenic component of water retention anyway. Better not to use them at all. Their use can only be reserved for those who (often, even if they do not take anything) have really high estrogen levels (above 40 pg / ml, as confirmed by a blood test that still takes it) and suffer from delay
- Diet Monitoring . Of course, if you limit the amount of carbohydrates, the delay disappears, but it doesn’t make sense if you are in the mass phase. Better to limit your sodium intake with a computerized diet: I say, limit, don’t rule out, because if you eat too little you will lose potassium, and even then you will have a blessed rebound (due to overproduction of the sodium-friendly hormone aldosterone ) and you would be very bloated like frogs if you eat food rich in salt. Instead of salt, limiting water intake, which is more than dangerous, is completely useless (the body sets up systems to retain even the small amount that you must take).
Finally, among natural systems, the most effective and beneficial is undoubtedly the regular practice of aerobic activities such as running or cycling, which, unfortunately, almost no one does. Those who tend to suffer from retention should gradually practice aerobics (not dance!) And stay in training. It is not true that running makes you lose muscle; it only does so if, due to too low aerobic fitness (where you are, of course, if you are doing weights only), you increase your running doses too quickly.
And the last, the last word for women: I leave aside the debate about whether women should be muscular or rather flexible and slim (soft, tough, etc.). From a purely medical point of view, a woman who really wants to take an anabolic should definitely do it under the strict supervision of a specialist doctor (endocrinologist), since ultimately these are male hormones. In addition to the side effects associated with more or less pronounced masculinization, there is a risk of damage to all female functions (menstruation, possibility of pregnancy) due to their very delicate nature.
Read more about this article
I liked this article primarily because it focuses on aspects of AAS danger that are usually ignored: we usually only deal with the axis, pituitary, gynuids and liver. But no one has ever died of hypogonadism, and even cases of liver tumors are indeed rare and statistically insignificant. Instead, it’s clear that premature deaths from heart attacks are more common among bodybuilders. The fact that bomber jackets are the least affected by cancer in the US population does not permit myocardial suicide.However, to make prevention as effective as possible, it is good to be as precise as possible, so two more words on how negative is expressed. the effect of AAS on lipids; is an effect that, in addition to being dose dependent, is formulated differently according to certain characteristics of the AAS:
- alkylates show the ability to worsen the HDL / LDL ratio at any dosage, even if they sometimes lower total cholesterol (especially oxandrolone and furazabol);
- unalkylated, on the other hand, exhibit this effect only at various high doses, depending on the specific substance, with non-flavorants, which exhibit this attitude at lower doses than with flavored; even fragrances have the paradoxical effect of improving lipids at the lowest doses.
For example, testosterone enanthate at a dose of 100 mg per week shows a clear lipid-enhancing effect, which, although decreasing, still remains at 300 mg; at 600 mg it leaves them unchanged, and at 900 the negative effect is evident. Probably, in men suffering from hypogonadism, this data will have to be slightly retouched upwards. For the prostate, I would be less alarmist: it is now established that benign hypertrophy is caused by estrogens and progestins, while for malignant there is no evidence of a connection with androgens: the experiment that started this dogma was from 1941 and is completely unreliable for the methods of execution and also for the partial report to which he was subject. In the case of women, the discussion goes against the usual discussion in men of not only fertility loss, which is sometimes welcome, but also the specific dependence of female hormones and the positive effects that AAS can have. in counteracting those psycho-nutritional disorders that women are more likely to experience
Let’s pause for a moment to think about the side effects, which are arguably the worst of the short term. As for the sexual ones, you think they are an advantage.
We say yes, but I must remember that an increase in libido, if not satisfied (Freud teaches …), can transform into other types of drives, up to before the crime. Finally, remember that an initial increase inevitably follows a decrease after suspension for the physiological reasons explained above. When it comes to the impact on aggression, I remember that they often wish bodybuilders or powerlifters to go to the gym more busy to lift huge weights. I do not deny that it is effective, but at what cost! If you really feel like you need the extra nerve to gain weight, it can mean many things, for example:
- You are probably mildly overtrained or the routine is boring and unproductive;
- You have other psychological problems;
- You are not made for this sport;
- In all the above cases, you are still wrong.
Dealing with these anabolic psychological “disorders” is absurd; It is better to act at the root of the problem, eliminate harmful causes and learn to control your mind, how to control your muscles. There are special methods for all this (self-hypnosis, autogenic training). As for other anabolic steroids, it should be said that their effect on libido and aggression seems to be related to the degree of androgenicity: from my own experience I have even seen that few androgenic products (eg winstrol) some subjects have a tendency to even decrease libido when used alone: however, this should not be dependent on a decrease in gonadotropins.
Now let’s look at some other effects not necessarily related to the androgenicity of products. . These include:
- Altered blood sugar . Androgenic anabolic agents can increase insulin sensitivity, this usually does not lead to hypoglycemia, but to a possible increase in its effects, that is, increase in fat, water retention, etc. These phenomena seem to be more pronounced in drugs that are sensitive to peripheral aromatization.
- Modification of blood lipids (fats)
Let’s pause for a moment to think about the side effects, which are arguably the worst of the short term. As for the sexual ones, you think they are an advantage.
We say yes, but I must remember that an increase in libido, if not satisfied (Freud teaches …), can transform into other types of drives, up to before the crime. Finally, remember that an initial increase inevitably follows a decrease after suspension for the physiological reasons explained above. When it comes to the impact on aggression, I remember that they often wish bodybuilders or powerlifters to go to the gym more busy to lift huge weights. I do not deny that it is effective, but at what cost! If you really feel that you need the extra nerve to gain weight, it can mean many things, for example:Dealing with these anabolic psychological “disorders” is absurd; It is better to act at the root of the problem, eliminate harmful causes and learn to control your mind, how to control your muscles. For all this, there are special methods (self-hypnosis, autogenous training).
As for other anabolic steroids, it should be said that their effect on libido and aggression, apparently, is associated with the degree of androgenicity: from my own experience, I have even seen that few androgenic foods (eg winstrol) tend to reduce libido in some subjects when used alone: however, this should not be dependent on a decrease in gonadotropins.
Now let’s look at some other effects not necessarily related to the androgenicity of foods .
Between this we remember:Let’s pause for a moment to think about the side effects, which are arguably the worst of the short term. Sexuals do you think they are an advantage.
We say yes, but I must remember that an increase in libido, if it is not satisfied (Freud teaches …), can be transformed into other types of drives, up to crime. Finally, remember that an initial increase inevitably follows a decrease after suspension for the physiological reasons explained above. When it comes to the impact on aggression, I remember that they often wish bodybuilders or powerlifters to go to the gym more busy to lift huge weights. I do not deny that it is effective, but at what cost! If you really feel like you need the extra nerve to gain weight, it can mean many things, for example:- You are probably mildly overtrained or the routine is boring and unproductive;
- You have other psychological problems;
- You are not made for this sport;
- In all the above cases, you are still wrong.
Dealing with these anabolic psychological “disorders” is absurd; It is better to act at the root of the problem, eliminate harmful causes and learn to control your mind, how to control your muscles. There are special methods for all this (self-hypnosis, autogenous training). As for other anabolic steroids, it should be said that their effect on libido and aggression seems to be related to the degree of androgenicity: from my own experience, I have even seen that few androgenic products (e.g. winstrol) tend to even decrease libido in some subjects when used alone: however, this should not be dependent on a decrease in gonadotropins.
Now let’s look at some other effects, not necessarily related to the androgenicity of foods. These include:
- Altered blood sugar … Androgenic anabolic agents can increase insulin sensitivity, this usually does not lead to hypoglycemia, but to a possible increase in its effects, that is, increase in fat, water retention, etc. These phenomena seem to be more pronounced in drugs that are sensitive to peripheral aromatization.
- Modification of blood lipids (fats) . I will dwell on this aspect for a moment, among the latter to be discovered. Androgenic-anabolic substances tend to reduce triglyceride levels by reducing the concentration of very low density lipoproteins (VLDL): this effect, in itself positive, is inherent in some derivatives of the progestogen nortestosterone, partly the same durabolin, oxandrolone, etc. However, over the past 5 years, they have been found to dramatically lower high-density lipoprotein levels, which carry the “good” portion of cholesterol (that is, HDL, which is the one that clears the arteries), and instead raise cholesterol levels associated with LDL lipoproteins (which Clog the arteries, predisposing to atherosclerosis).
And think that they were even used to treat hypertriglyceridemia! The effect does not depend on the dose, but, by blocking a certain enzymatic pathway, it appears already in small doses, and sometimes within just 2 days. All drugs, regardless of their characteristics (androgenicity, aromatization), seem to share it. Now, this side effect (along with the hypertension, which I will continue about) is the most dangerous mean to me. Not noticing that nothing (while acne and water retention become clearly visible), the arteries become blocked.It cannot be said that atherosclerosis affects all those who take anabolic drugs, but there is no doubt that the risk increases enormously, and not in a probabilistic way ( such as smoking – lung cancer), but much more direct, that is, associated with the duration of… What is usually the first sign of atherosclerosis in a relatively young subject? It is easy to say: death from a heart attack. In the following years, the manifestations, although very serious, become more treatable (with medication, surgery, etc.), but I think you all know what it means to suffer from the heart. Other complications occur at an older age (60-70 years) on the kidneys, brain, etc. Therefore, please do not say that “those who take anabolic are healthy like fish” or something like that: it seems as healthy as a fish, but his arteries are very likely to be destroyed, and would be curious to know if in middle age, especially when you stop exercising, I still feel so good.
Tendency to water retention and hypertension . This side effect is partly dependent on estrogen, but also on the androgen effect itself and / or on the effect on insulin (see above) or endogenous cortisone, all hormones that cause water retention. Water retention in the uninitiated is manifested by edema, especially on the face, ankles; then the bodybuilder, who usually looks in the mirror, will notice the often conspicuous definition, even if the body fat remains the same, that is, it is “smoothed”. Water retention can be roughly measured with a balance: weight that increases rapidly (2-3 days) and disappears just as quickly when the drug is discontinued is nothing more than water retention.Obviously, the most androgenic and flavored foods (testosterone , dianabol, boldenone) are given almost always, even depending on the dose; much less androgenic (methandriol, especially deca) and even less non-aromatized androgens (winstrol, oxandrolone, primobolan)… Of course, it is common knowledge that the ease with which water is retained, even with equal doses of the same drug, varies greatly from person to person, as do all side effects in general: as a rule, people with a tendency to slow metabolism retain more water, probably because Under these conditions, the transformation of steroids is more focused on the production of estrogen (through metabolic 5-beta reduction) than other products (through 5-alpha), and also because the metabolism of cortisol itself is slowed down. Finally, in the same person, the delay is much more apparent with a free diet (carbohydrates) than with a very limited diet. In some cases, retention does not present any other obvious problem besides aesthetic; in others, it is accompanied by an increase in blood pressure. In young and healthy people, the increase in pressure can only be temporary (for several days), because later the mechanisms of self-regulation, as a rule, return it to its place; but in some cases the pressure remains high. Therefore, it is almost imperative that every good gym has a sphygmomanometer, perhaps an automatic type, so that all those who do weight (anabolic or not) can check themselves regularly. Remember that those with very large hands may have falsely higher values of 10-15 mmHg. Art.
Gynecomastia . This means the appearance, to a large extent, of tissue similar to a woman’s breasts in the area behind the nipple. This phenomenon is easily distinguishable from “boobs” in obese males (when the swelling occurs from adipose tissue, and not from the mammary glands), this phenomenon is observed physiologically almost in half of the adolescents, and then disappears. This is naturally due to estrogen. Highly androgenic and aromatized steroids (as well as a diuretic commonly used by bodybuilders, spironolactone or aldactone) can also cause it in adults if taken in excessive doses for extended periods of time… If you allow it to develop, this defect, often even painful, will unfortunately become irreversible (surgery is required).
Liver toxicity . In the past, this has been the most famous side effect of anabolic steroids. In fact, testosterone itself is not toxic to the liver at all, on the contrary, it helps limit the damage it undergoes from numerous toxic substances (alcohol, etc.), so much so that it was once used as an adjuvant in the treatment of liver cirrhosis … The same goes for derivatives. The toxicity attributed to steroids does not depend on the fact that they are steroids, but on the molecular change (alkylation at the 17-alpha position) that many of them have, that is, “traditional” oral. Some injectable drugs are also 17-alpha alkylated (winstrol, methandriol), which is a controversy because alkylation is necessary to prolong the life of orally administered drugs in the body (otherwise the liver will eliminate them immediately). The toxicity of alkylates, as always, depends on time and dose. The first signs consist of inflammation of the bile ducts with jaundice, at first not obvious, and then clinical (the sclera, that is, the white parts of the eyes, are the first areas where jaundice is observed), then an increase in the level of Gamma Gt in the blood. then SGOT and finally SGPT. Many malignant liver tumors (hepatomas) have been attributed to the use of these products, unfortunately, also in bodybuilders.Of course, those who want to check their luggage will say that the tests are not definitive, but in the face of even one similar risk I would say that both it is probably best to avoid taking alkylates that have similar or identical non-toxic liver products.
Finally, another effect of anabolic agents has been attributed to 17-alpha-alkylation, namely the anticoagulant effect… In fact, due to increased fibrinolysis (i.e., the clot is easier to remove), this phenomenon is also observed with non-alkylated products such as ethylestrenol and nandrolones (deca-durabolin). Unless the person has had preexisting coagulation changes, this effect is relatively harmless.
What are the therapeutic indications for these drugs?
Their androgenic characteristics are mainly used to maintain or develop sexual characteristics in cases of deficiency; anabolic performance in case of protein depletion. But let’s see what is mainly used:- In case of infertility due to azoospermia (i.e. a decrease in sperm count).
- Conditions of low sexual potency (even if due to psychological reasons) can be treated with androgens (typically up to 200 mg / week) given their well-documented role in libido development and maintenance.
- In some cases of breast cancer in women, they are used to curb (unfortunately only palliatively) the development of cancer and pain, in this case, non-aromatized androgens are preferably used in doses that must necessarily be higher than in men: subsequent virilization tolerable given the severity of the disease.
- Anabolic agents have instead been used in cases of protein malnutrition in adults and incorrectly in children (see the case of Dianabol). They improve appetite and, together with proper nutrition, stimulate protein synthesis.
- Similarly, they are used in certain preoperative conditions to improve the trophism of the patient due to severe stress or after the operation itself to facilitate recovery during the recovery period; for the same reason they have been used in severely injured patients or, more generally, in patients forced to lie in bed for extended periods of time to reduce protein catabolism due to stress and / or non-use.
- They are used for severe burns to stimulate faster repair of damaged tissue.
- They are now widely used in the treatment of osteoporosis in both sexes to stimulate bone protein matrix formation and calcium deposition.
- They are often associated with cortisone drugs in chronic therapy to minimize the catabolic effects of these drugs (highly visible on bone, muscle, skin, etc.).
- They are also sometimes used in cases of arthritis or arthrosis and other chronic conditions.
- Finally, for aplastic anemias (that is, those not associated with vitamin B12 or folic acid deficiencies), they were used in very strong doses (before testosterone was used, then we switched to an anabolic drug such as decadurabolin, so as it was seen that the effectiveness was the same, with fewer side effects).
Obviously the average athlete doesn’t get into any of these cases (hopefully); why then do you use anabolic steroids?
Through their use we are trying to stimulate protein synthesis to increase muscle mass and strength, or in resistance to prolonged effort in middle distance athletes. However, the scientific community has not yet been able to demonstrate the effectiveness of these drugs as ergogenic, due in part to the stringency of criteria commonly used in research protocols. Many authors believe that every beneficial effect attributed to steroids is in fact related to the so-called “effect placebo ”(that is, to believe that the substance is good, followed by an improvement in training, etc., in the particular case of the athlete). .
I will cite two of the best studies in this area:- Fowler et al. in a double-blind study (neither they nor the athletes knew who was taking the placebo or who was taking the drug) tested 47 students aged 28 to 25… 10 were footballers, so athletes trained, the rest were not. Six groups were made (players with half placebos and half drugs, sedentary or not, drug or placebo). Androstenolone was used at a dose of 20 mg per day for 16 weeks. Neither group experienced significant increases in weight, strength, or muscle mass.
- Casner et al conducted a 1971 study on the effect of Winstrol on 27 college students. There were also 4 groups made here: students with placebo or drugs and with or without (resistance) training. Among the parameters measured was a significant increase in body weight in those taking Winstrol, which means that they gained more weight than the placebo. Further analysis, however, appears to make it clear that the weight gain was associated with water retention and not with actual gains in muscle mass. Even here, according to the authors, there was no reason for the use of anabolic steroids in athletes.
HOW TO MINIMIZE SIDE EFFECTS
Unfortunately, those who have decided to take or are already taking anabolic medications will not (I’m afraid) be convinced or intimidated by the above. Although, of course, I do not recommend taking these substances from a medical point of view for the sole purpose of improving athletic performance, of course, many will continue to take them. And therefore it must be said for them that it is also true that, like any other medicine, the frequency of side effects can truly be minimized if the bodybuilder uses steroids correctly. And let’s see how.
Of course, the dose used is a critical factor: let’s explain why with a few small pharmacology notes.
Each drug has the desired action (main effect). At a certain “threshold” dose, nothing happens. Above this dose, the effect manifests itself and increases with increasing dose in an indirect way (i.e…. does not triple when the dose is tripled), but is usually logarithmic. Upon reaching a certain dose, the effect no longer increases, if not insignificantly (property of logarithms), even at doses tens of times higher. Various side effects also have a “range” of reaction, often different from the main effect.Let’s take testosterone as an example.
Less than 15 mg / week, each effect is minimal. Already at 35 mg / week, a clear nitrogen retention effect is observed. There is no water retention or marked inhibition of gonadotropins at these doses (side effects). By gradually increasing the dose, we will have from 40 to 200 mg per week, first partial and then complete inhibition of gonadotropins. The nitrogen retention effect reaches almost maximum at 200 mg / week, the well-known effect is only twice as high as with a 5-fold reduced dose.
At 400 mg / week, nitrogen retention no longer increases and instead it is clear that water one.
Finally, at doses over 1000 mg (once used to treat certain anemias), virilization and retention are intrusive.
Thus, careful use of a drug that plays at doses already makes a difference.Another factor related to dose size is the length of the dose period. The discussion is similar to the previous one, Each effect takes its own time.
Water and salt retention is a rather fast process (2-3 days), carbohydrates and potassium are slower, phosphorus is slower (months) and nitrogen is bound to even slower contractile proteins. Inhibition of spermatogenesis is completed in 3-5 months. Then “virilization” (apparently in children and women) occurs very slowly and, as you know, ends in years, not months. The concept of reversibility is also related to duration of action. Virilization is known to be almost irreversible; atherosclerosis is very small if caught early.It follows from all this that medications, as a rule, should be taken in the shortest possible time necessary for building muscle proteins. Experience shows that a good anabolic effect is achieved after 4-6 weeks: at these doses, testicular atrophy and serum lipid modification are rather scarce.
The concept of dose is perhaps even more important in the case of low androgenic anabolic substances, which, as mentioned at the beginning are usually true at low doses. and they become more androgenic at higher doses. Using steroids that are too high and causing more side effects will only increase your risk of becoming “insensitive” to the drug itself. This phenomenon, typical of endocrinology, may be due to the fact that the cellular structures responsible for recognizing steroids and receiving the message of war (receptors) decrease in number if they are exposed for a long time to too high concentrations of the same, as to protect cells from overdose.
This phenomenon is called down-regulation (sub-regulation) and is also typical of thyroid hormones (beware !!!), insulin and other hormones ..
Well, many so-called drug formulators believe that switching from one steroid to another is a method of eliminating downregulation.
You won’t believe that mother nature has created as many different types of receptors as there are steroids. on the market! There is only one steroid receptor, and if it decreases, the effect of any anabolic steroid will decrease. It also follows how wrong another typical bodybuilding practice is: stacking (using two or more steroids together) or even “bombarding” (megadoses of different drugs, type 100 deca, 200 testosterone, 200 primobolan … per day!): If the receptor ( poor guy) only one, you only put it in your underwear.
Rather, it must be said that just because the receptor is the same does not mean that different foods have the same effect. In fact, once inside the cell, the steroid can be metabolized in different ways (I mentioned this earlier), causing different effects: c. for example, a more noticeable increase in phosphocreatine and mitochondria for a more androgenic (“massive” effect), a more noticeable increase in contractile proteins for a less androgenic (“power” effect), etc.
I advise you to re-read well what I wrote and keep this in mind. During steroid therapy (and even after its termination) it would be good to check at least the following indicators:- pressure once a week
- Body weight every day (an increase of more than 1 kg per week is an undeniable indicator of water retention)
- A in the blood – SGOT, SGPT, Gamma-Gt, bilirubins, total cholesterol, triglycerides and HDL cholesterol (or protein electrophoresis).
- Every 3-6 months, especially if you are under strong androgen, you should have a rectal exam.
It is not advisable to bring these tests to your doctor, unless he is an expert in the field and is not friendly with you, Seek a doctor who knows the environment and whom you trust to help you interpret the tests in light the fact that you are taking steroids.
If, at last, side effects appear, what to do? I have to say this on an individual basis. However, in general I would say:
- If liver enzymes (SGOT, SGPT, Gamma-Gt or Bilirubin) change, stop using 17-alpha alkylates (Winstrol, Oxandrolon abnehmen, Dianabol, etc.) and forget about them for the rest of your life. If you didn’t take them instead, it’s very likely that you have real liver disease, regardless of steroids..
- If you have a tendency to have low HDL cholesterol levels even in normal conditions and / or family members (dad, uncle, grandparents) with a history of heart attack, check this index very carefully and, if you really need to, do short cycles. Then try (but that’s even if you’re not on steroids) regularly aerobics throughout your life (that’s not what I’m talking about in terms of sports prevention, I’m not talking here).
- In case of acne, avoid ignoring it until you become a leper. Miracles don’t work here, just: a) avoid using highly androgenic products and do not exceed therapeutic doses b) cleanse your skin properly and use antibiotic ointments (although acne, although androgens prefer them, is a bacterial infection) c) try to stay in the sun if it is possible.
- In the case of gynecomastia, you will almost always find testosterone or dianabol responsible. Well, all you have to do is stop them and you won’t have to take any more flavored drugs.
- In the event of excessive (for your usual purposes) water retention, reduce the doses and you will see this phenomenon almost always subside. If this continues, be aware that there are other ways to reduce water retention, many of which are possibly worse than water retention ..
One more article is required for their exhaustive consideration, so I will only mention:
- Diuretics : they deplete salts, the effect is often uncontrollable, and if you really need to, use them for several days (and with appropriate supplementation) of minerals, which is strictly dependent on the diuretic or combinations of diuretics used). They can be very dangerous (if not for life, of course for a sports presentation: consider doing weight or doing cramps racing …)… However, diuretics were recently banned from IFBB racing.
- Antiestrogens : (tamoxifen or nolvadex, testonolactone and testolac, cyclophenyl). They are quite toxic drugs in the long run; they tend to give a slurry rebound effect (that is, when you stop them, you swell like balls), and this only acts on the estrogenic component of water retention anyway. Better not to use them at all. Their use can only be reserved for those who (often, even if they do not take anything) have really high estrogen levels (above 40 pg / ml, as confirmed by a blood test that still takes it) and suffer from delay
- Diet Monitoring . Of course, if you limit the amount of carbohydrates, the delay disappears, but it doesn’t make sense if you are in the mass phase. Better to limit your sodium intake with a computerized diet: I say, limit, don’t rule out, because if you eat too little you will lose potassium, and even then you will have a blessed rebound (due to overproduction of the sodium-friendly hormone aldosterone ) and you would be very bloated like frogs if you eat food rich in salt. Instead of salt, limiting water intake, which is more than dangerous, is completely useless (the body sets up systems to retain even the small amount that you must take).
Finally, among natural systems, the most effective and beneficial is undoubtedly the regular practice of aerobic activities, such as running or cycling, which, unfortunately, almost no one does. Those who tend to suffer from retention should gradually engage in aerobics (not dance!) And stay in training… It is not true that running makes you lose muscle; it only does so if, due to too low aerobic fitness (where you are, of course, if you are doing weights only), you increase your running doses too quickly.
And the last, the last word for women: I leave aside the debate about whether women should be muscular or rather flexible and slim (soft, tough, etc.). From a purely medical point of view, a woman who really wants to take an anabolic should definitely do it under the strict supervision of a specialist doctor (endocrinologist), since ultimately these are male hormones. In addition to the side effects associated with more or less pronounced masculinization, there is a risk of damage to all female functions (menstruation, possibility of pregnancy) due to their very delicate nature.
Read more about this article
I liked this article primarily because it focuses on aspects of AAS danger that are usually ignored: we usually only deal with the axis, pituitary, gynuids and liver. But no one has ever died of hypogonadism, and even cases of liver tumors are indeed rare and statistically insignificant. Instead, it’s clear that premature deaths from heart attacks are more common in bodybuilders…. The fact that bomber jackets are the least affected by cancer in the US population does not permit myocardial suicide.However, to make prevention as effective as possible, it is good to be as precise as possible, so two more words on how negative is expressed. the effect of AAS on lipids; is an effect that, in addition to being dose dependent, is formulated differently according to certain characteristics of the AAS:
- alkylates show the ability to worsen the HDL / LDL ratio at any dosage, even if they sometimes lower total cholesterol (especially oxandrolone and furazabol);
- unalkylated, on the other hand, exhibit this effect only at various high doses, depending on the specific substance, with non-flavorants, which exhibit this attitude at lower doses than with flavored; even fragrances have the paradoxical effect of improving lipids at the lowest doses.
For example, testosterone enanthate at a dose of 100 mg per week shows a clear lipid-enhancing effect, which, although decreasing, still remains at 300 mg; at 600 mg it leaves them unchanged, and at 900 the negative effect is evident. Probably, in men suffering from hypogonadism, this data will have to be slightly retouched upwards. For the prostate, I would be less alarmist: it is now established that benign hypertrophy is caused by estrogens and progestins, while for malignant there is no evidence of a connection with androgens: the experiment that started this dogma was from 1941 and is completely unreliable for the methods of execution and also for the partial report to which he was subject. For women, the discussion goes against the usual discussion in men of not only fertility loss, which is sometimes welcome, but also the specific dependence of female hormones, as well as the positive effects that AAS can have…. in counteracting those psycho-nutritional disorders that women are more likely to experience
Let’s pause for a moment to think about the side effects, which are arguably the worst of the short term. As for the sexual ones, you think they are an advantage.
We say yes, but I must remember that an increase in libido, if not satisfied (Freud teaches …), can transform into other types of drives, up to before the crime. Finally, remember that an initial increase inevitably follows a decrease after suspension for the physiological reasons explained above. When it comes to the impact on aggression, I remember that they often wish bodybuilders or powerlifters to go to the gym more busy to lift huge weights. I do not deny that it is effective, but at what cost! If you really feel like you need the extra nerve to gain weight, it can mean many things, for example:- You are probably mildly overtrained or the routine is boring and unproductive;
- You have other psychological problems;
- You are not made for this sport;
- In all the above cases, you are still wrong.
Dealing with these anabolic psychological “disorders” is absurd; It is better to act at the root of the problem, eliminate harmful causes and learn to control your mind, how to control your muscles. There are special methods for all this (self-hypnosis, autogenous training). As for other anabolic steroids, it should be said that their effect on libido and aggression seems to be related to the degree of androgenicity: from my own experience, I have even seen that few androgenic products (such as winstrol) in some subjects there is a tendency to decrease even libido if used alone: however, this should not be dependent on a decrease in gonadotropins.
Now let’s look at some other effects, not necessarily related to the androgenicity of foods. These include:- Altered blood sugar . Androgenic anabolic agents can increase insulin sensitivity, this usually does not lead to hypoglycemia, but to a possible increase in its effects, that is, increase in fat, water retention, etc. These phenomena seem to be more pronounced in drugs that are sensitive to peripheral aromatization.
- Modification of blood lipids (fats) . I will dwell on this aspect for a moment, among the latter to be discovered. Androgenic-anabolic substances tend to reduce triglyceride levels by reducing the concentration of very low density lipoproteins (VLDL): this effect, in itself positive, is inherent in some derivatives of the progestogen nortestosterone, partly the same durabolin, oxandrolone, etc. However, over the past 5 years, they have been found to dramatically lower high-density lipoprotein levels, which carry the “good” portion of cholesterol (that is, HDL, which is the one that clears the arteries), and instead raise cholesterol levels associated with LDL lipoproteins (which “Pollute” the arteries, causing a predisposition to atherosclerosis). And think that they were even used to treat hypertriglyceridemia! The effect does not depend on the dose, but, by blocking a certain enzymatic pathway, it appears already in small doses, and sometimes within just 2 days. All drugs, regardless of their characteristics (androgenicity, aromatization), seem to share it. Now, this side effect (along with the hypertension, which I will continue about) is for me the most dangerous vile… Without noticing that nothing (while acne and water retention become clearly visible), the arteries become blocked, It cannot be said that atherosclerosis affects all those who take anabolic drugs, but it is undoubted that the risk increases enormously, and not in a probabilistic way ( such as smoking – lung cancer), but much more direct, that is, associated with the duration of intake. What is usually the first sign of atherosclerosis in a relatively young subject? It is easy to say: death from a heart attack. In the following years, the manifestations, although very serious, become more treatable (with medication, surgery, etc.), but I think you all know what it means to suffer from the heart. Other complications occur at an older age (60-70 years) on the kidneys, brain, etc. Therefore, please do not say that “those who take anabolic are healthy as fish” or something like that: it seems healthy as a fish, but his arteries are very likely to be destroyed, and would be curious to know if middle age, especially when you stop exercising, still feel so good.
- Tendency to water retention and hypertension . This side effect is partly dependent on estrogen, but also on the androgen effect itself and / or on the effect on insulin (see above) or endogenous cortisone, all hormones that cause water retention. Water retention in the uninitiated is manifested by edema, especially on the face, ankles; then the bodybuilder, who usually looks in the mirror, will notice the often conspicuous definition, even if the body fat remains the same, that is, it is “smoothed”… Water retention can be roughly measured with a balance: weight that increases rapidly (2-3 days) and disappears just as quickly when the drug is discontinued is nothing more than water retention.Obviously, the most androgenic and flavored foods (testosterone , dianabol, boldenone) are given almost always, even depending on the dose; much less small androgens (methandriol, especially deca) and even less small non-aromatized androgens (winstrol, oxandrolone, primobolan). Of course, it is common knowledge that the ease with which water is retained, even with equal doses of the same drug, varies greatly from person to person, as do all side effects in general: as a rule, people with a tendency to slow metabolism retain more water, probably because Under these conditions, the transformation of steroids is more focused on the production of estrogen (through metabolic 5-beta reduction) than other products (through 5-alpha), and also because the metabolism of cortisol itself is slowed down. Finally, in the same person, the delay is much more apparent with a free diet (carbohydrates) than with a very limited diet. In some cases, retention does not present any other obvious problem besides aesthetic; in others, it is accompanied by an increase in blood pressure. In young and healthy people, the increase in pressure can only be temporary (for several days), because later the mechanisms of self-regulation, as a rule, return it to its place; but in some cases the pressure remains high. Therefore, it is almost imperative that every good gym has a sphygmomanometer, perhaps an automatic type, so that all those who do weight (anabolic or not) can check themselves regularly. Remember that those with very large hands may have falsely higher values of 10-15 mm / Hg. Art.
- gynecomastia … This means the appearance, to a large extent, of tissue similar to a woman’s breasts in the area behind the nipple. This phenomenon is easily distinguishable from “boobs” in obese males (when the swelling occurs from adipose tissue, and not from the mammary glands), this phenomenon is observed physiologically almost in half of the adolescents, and then disappears. This is naturally due to estrogen. Highly androgenic and aromatized steroids (as well as a diuretic commonly used by bodybuilders, spironolactone or aldactone) can also cause it in adults if taken in excessive doses for extended periods of time. If you allow it to develop, this defect, often even painful, unfortunately, will become irreversible (surgery is required).
- Liver toxicity . In the past, this has been the most famous side effect of anabolic steroids. In fact, testosterone itself is not toxic to the liver at all, on the contrary, it helps limit the damage it undergoes from numerous toxic substances (alcohol, etc.), so much so that it was once used as an adjuvant in the treatment of liver cirrhosis … The same goes for derivatives. The toxicity attributed to steroids does not depend on the fact that they are steroids, but on the molecular change (alkylation at the 17-alpha position) that many of them have, that is, “traditional” oral. Some injectable drugs are also 17-alpha alkylated (winstrol, methandriol), which is a controversy because alkylation is necessary to prolong the life of orally administered drugs in the body (otherwise the liver will eliminate them immediately). The toxicity of alkylates, as always, depends on time and dose. The first signs consist of inflammation of the bile ducts with jaundice, at first not obvious, and then clinical (the sclera, that is, the white parts of the eyes, are the first areas where jaundice is observed), then an increase in the level of Gamma Gt in the blood. then SGOT and finally SGPT… Many malignant liver tumors (hepatomas) have been attributed to the use of these products, unfortunately, also in bodybuilders.Of course, those who want to check their luggage will say that the tests are not definitive, but in the face of even such a risk I would say that how can rather, it is best to avoid taking alkylates that have similar or identical non-toxic liver products.
Finally, another effect of anabolic agents has been attributed to 17-alpha-alkylation, namely the anticoagulant effect. In fact, due to increased fibrinolysis (i.e., the clot is easier to remove), this phenomenon is also observed with non-alkylated products such as ethylestrenol and nandrolones (deca-durabolin). Unless the person has had any pre-existing coagulation changes, this effect is relatively harmless.
What are the therapeutic indications for these drugs?
Their androgenic characteristics are mainly used to maintain or develop sexual characteristics in cases of deficiency; anabolic performance in case of protein depletion. But let’s see what is mainly used:- In case of infertility due to azoospermia (i.e. a decrease in sperm count).
- Conditions of low sexual potency (even if due to psychological reasons) can be treated with androgens (usually up to 200 mg / week) given their well-documented role in the development and maintenance of libido.
- In some cases of breast cancer in women, they are used to curb (unfortunately only palliatively) the development of cancer and pain, in this case, non-aromatized androgens are preferably used in doses that must necessarily be higher than in men: subsequent virilization tolerable given the severity of the disease.
- Anabolic agents have instead been used in cases of protein malnutrition in adults and incorrectly in children (see… the case of Dianabol), They improve appetite and, together with proper nutrition, stimulate protein synthesis.
- Similarly, they are used in certain preoperative conditions to improve the trophism of the patient due to severe stress or after the operation itself to facilitate recovery during the recovery period; for the same reason they have been used in severely injured patients or more generally in patients who have to lie in bed for extended periods of time to reduce protein catabolism due to stress and / or disuse.
- They are used for severe burns to stimulate faster repair of damaged tissue.
- They are now widely used in the treatment of osteoporosis in both sexes to stimulate bone protein matrix formation and calcium deposition.
- They are often associated with cortisone drugs in chronic therapy to minimize the catabolic effects of these drugs (highly visible on bone, muscle, skin, etc.).
- They are also sometimes used in cases of arthritis or arthrosis and other chronic conditions.
- Finally, for aplastic anemias (that is, those not associated with vitamin B12 or folic acid deficiencies), they were used in very strong doses (before testosterone was used, then we switched to an anabolic drug such as decadurabolin, so as it was seen that the effectiveness was the same, with fewer side effects).
Obviously the average athlete doesn’t get into any of these cases (hopefully); why then do you use anabolic steroids?
Through their use we are trying to stimulate protein synthesis to increase muscle mass and strength, or resistance to prolonged effort in middle distance athletes… However, the scientific community has not yet been able to demonstrate the effectiveness of these drugs as ergogenic, due in part to the stringency of criteria commonly used in research protocols. Many authors believe that every beneficial effect attributed to steroids is in fact related to the so-called “effect placebo ”(that is, to believe that the substance is good, followed by an improvement in training, etc., in the particular case of the athlete). .
I will cite two of the best studies in this area:- Fowler et al. in a double-blind study (neither they nor the athletes knew who was taking the placebo or who was taking the drug) tested 47 students between the ages of 28 and 25. 10 were footballers, so athletes trained, the rest were not. Six groups were made (players with half placebos and half drugs, sedentary or not, drug or placebo). Androstenolone was used at a dose of 20 mg per day for 16 weeks. Neither group experienced significant increases in weight, strength, or muscle mass.
- Casner et al conducted a 1971 study on the effect of Winstrol on 27 college students. There were also 4 groups made here: students with placebo or drugs and with or without (resistance) training. Among the parameters measured was a significant increase in body weight in those taking Winstrol, which means that they gained more weight than the placebo. Further analysis, however, appears to make it clear that the weight gain was associated with water retention and not with actual gains in muscle mass. Even here, according to the authors, there was no reason for the use of anabolic steroids in athletes.
HOW TO MINIMIZE SIDE EFFECTS
Unfortunately, those who have decided to take or are already taking anabolic medications will not (I am afraid) be convinced or afraid of the above… Although, of course, I do not recommend taking these substances from a medical point of view for the sole purpose of improving athletic performance, of course, many will continue to take them. And therefore it must be said for them that it is also true that, like any other medicine, the frequency of side effects can truly be minimized if the bodybuilder uses steroids correctly. And let’s see how.
Of course, the dose used is a critical factor: let’s explain why with a few small pharmacology notes.
Each drug has the desired action (main effect). At a certain “threshold” dose, nothing happens. Above this dose, the effect manifests itself and increases with increasing dose indirectly (i.e., it does not triple when the dose is threefold), but is usually logarithmic. Upon reaching a certain dose, the effect no longer increases, if not insignificantly (property of logarithms), even at doses tens of times higher. Various side effects also have a “range” of reaction, often different from the main effect.Let’s take testosterone as an example.
Less than 15 mg / week, each effect is minimal. Already at 35 mg / week, a clear nitrogen retention effect is observed. There is no water retention or marked inhibition of gonadotropins at these doses (side effects). By gradually increasing the dose, we will have from 40 to 200 mg per week, first partial and then complete inhibition of gonadotropins. The nitrogen retention effect reaches almost maximum at 200 mg / week, the well-known effect is only twice as high as with a 5-fold reduced dose.
At 400 mg / week, nitrogen retention no longer increases and instead it is clear that water one.
Finally, in doses greater than 1000 mg (once used to treat some anemias), virilization and retention is imposed. difference.Another factor related to dose size is the length of the dose period… The discussion is similar to the previous one, Each effect takes its own time.
Water and salt retention is a rather fast process (2-3 days), carbohydrates and potassium are slower, phosphorus is slower (months) and nitrogen is bound to even slower contractile proteins. Inhibition of spermatogenesis is completed in 3-5 months. Then “virilization” (apparently in children and women) occurs very slowly and, as you know, ends in years, not months. The concept of reversibility is also related to duration of action. Virilization is known to be almost irreversible; atherosclerosis is very small if caught early.It follows from all this that medications, as a rule, should be taken in the shortest possible time necessary for building muscle proteins. Experience shows that a good anabolic effect is achieved after 4-6 weeks: at these doses, testicular atrophy and serum lipid modification are rather scarce.
The concept of dose is perhaps even more important in the case of low androgenic anabolic substances, which, as mentioned at the beginning are usually true at low doses. and they become more androgenic at higher doses. Using steroids that are too high and causing more side effects will only increase your risk of becoming “insensitive” to the drug itself. This phenomenon, typical of endocrinology, may be due to the fact that the cellular structures responsible for recognizing steroids and receiving the message of war (receptors) decrease in quantity if they are exposed for a long time to too high concentrations of the same, as to protect the cell from overdose.
This phenomenon is called down-regulation (sub-regulation) and is also typical of thyroid hormones (beware !!!), insulin and other hormones ..
Well, many so-called formulators believe that switching from one steroid to another is a method of eliminating downregulation.
You won’t believe that mother nature has created as many different types of receptors as steroids. on the market! There is only one steroid receptor, and if it decreases, the effect of any anabolic steroid will decrease. It also follows how wrong another typical bodybuilding practice is: stacking (using two or more steroids together) or even “bombarding” (megadoses of different drugs, type 100 deca, 200 testosterone, 200 primobolan … per day!): If the receptor ( poor fellow) only one, you put it only in your underwear.
Rather, it must be said that if the receptor is the same, this does not mean that different products have the same effect. In fact, once inside the cell, the steroid can be metabolized in different ways (I mentioned this earlier), causing different effects: c. for example, a more noticeable increase in phosphocreatine and mitochondria for a more androgenic (“massive” effect), a more noticeable increase in contractile proteins for a less androgenic (“power” effect), etc.
I advise you to re-read well what I wrote and keep this in mind. During steroid therapy (and even after its termination) it would be good to check at least the following indicators:- pressure once a week
- Body weight every day (an increase of more than 1 kg per week is an undeniable indicator of water retention)
- A in the blood – SGOT, SGPT, Gamma-Gt, bilirubins, total cholesterol, triglycerides and HDL cholesterol (or protein electrophoresis).
- Every 3-6 months, especially if you are under strong androgen, you should have a rectal exam.
It is not advisable to bring these tests to your doctor, unless he is an expert in the field and is not friendly with you, Seek a doctor who knows the environment and whom you trust to help you interpret the tests in light the fact that you are taking steroids.
If, at last, side effects appear, what to do? I have to say this on an individual basis. However, in general I would say:
- If liver enzymes (SGOT, SGPT, Gamma-Gt or Bilirubin) change, stop using 17-alpha alkylates (Winstrol, Oxandrolone, Dianabol, etc.) and forget about them for the rest of your life. If you didn’t take them instead, it’s very likely that you have real liver disease, regardless of steroids.
- If you have a tendency to have low HDL cholesterol levels even in normal conditions and / or family members (dad, uncle, grandparents) with a history of heart attack, check this index very carefully and, if you really need to, do short cycles. Then try (but that’s even if you’re not on steroids) regularly aerobics throughout your life (that’s not what I’m talking about in terms of sports prevention, I’m not talking here).
- In the event of acne, avoid ignoring it until you become a leper. Miracles don’t work here, just: a) avoid using highly androgenic products and do not exceed therapeutic doses b) cleanse your skin properly and use antibiotic ointments (although acne, although androgens prefer them, is a bacterial infection) c) try to stay in the sun if it is possible.
- In the case of gynecomastia, you will almost always find testosterone or dianabol responsible. Well, all you can do is stop them and you won’t have to take any more flavored drugs.
- In the event of excessive (for your usual purposes) water retention, reduce the doses and you will see this phenomenon almost always subside. If this continues, be aware that there are other ways to reduce water retention, many of which are arguably worse than having it..
One more article is required for their exhaustive consideration, so I will only mention:
- Diuretics : they deplete salts, the effect is often uncontrollable, and if you really need to, use them for several days (and with appropriate supplementation) of minerals, which is strictly dependent on the diuretic or combinations of diuretics used). They can be very dangerous (if not for life, of course, for a sports presentation: consider doing weight or doing cramps racing …). However, diuretics were recently banned from IFBB racing.
- Antiestrogens : (tamoxifen or nolvadex, testonolactone and testolac, cyclophenyl). They are quite toxic drugs in the long run; they tend to give a slurry rebound effect (that is, when you stop them, you swell like balls), and this only acts on the estrogenic component of water retention anyway. Better not to use them at all. Their use can only be reserved for those who (often, even if they do not take anything) have really high estrogen levels (above 40 pg / ml, as confirmed by a blood test that still takes it) and suffer from delay
- Diet Monitoring . Of course, if you limit the amount of carbohydrates, the delay disappears, but it doesn’t make sense if you are in the mass phase. Better to limit your sodium intake with a computerized diet: I say, limit, don’t rule out, because if you eat too little you will lose potassium, and even then you will have a blessed rebound (due to overproduction of the sodium-friendly hormone aldosterone ) and you would be very bloated like frogs if you eat food rich in salt… Instead of salt, limiting water intake, which is more than dangerous, is completely useless (the body sets up systems to retain even the small amount that you must take).
Finally, among natural systems, the most effective and beneficial is undoubtedly the regular practice of aerobic activities, such as running or cycling, which, unfortunately, almost no one does. Those who tend to suffer from retention should gradually practice aerobics (not dance!) And stay in training. It is not true that running makes you lose muscle; it only does so if, due to too low aerobic fitness (where you are, of course, if you are doing weights only), you increase your running doses too quickly.
And the last, the last word for women: I leave aside the debate about whether women should be muscular or rather flexible and slim (soft, tough, etc.). From a purely medical point of view, a woman who really wants to take an anabolic should definitely do it under the strict supervision of a specialist doctor (endocrinologist), since ultimately these are male hormones. In addition to the side effects associated with more or less pronounced masculinization, there is a risk of damage to all female functions (menstruation, possibility of pregnancy) due to their very delicate nature.
- Propensity for water retention and hypertension
Let’s pause for a moment to think about the side effects, which are arguably the worst of the short term. As for the sexual ones, you think they are an advantage.
We say yes, but I must remember that an increase in libido, if not satisfied (Freud teaches …), can transform into other types of drives, up to before the crime. Finally, remember that an initial increase inevitably follows a decrease after suspension for the physiological reasons explained above. When it comes to the impact on aggression, I remember that they often wish bodybuilders or powerlifters to go to the gym more busy to lift huge weights. I do not deny that it is effective, but at what cost! If you really feel that you need the extra nerve to gain weight, it can mean many things, for example:Dealing with these anabolic psychological “disorders” is absurd; It is better to act at the root of the problem, eliminate harmful causes and learn to control your mind, how to control your muscles. For all this, there are special methods (self-hypnosis, autogenous training).
As for other anabolic steroids, it should be said that their effect on libido and aggression, apparently, is associated with the degree of androgenicity: from my own experience, I have even seen that few androgenic foods (eg winstrol) tend to reduce libido in some subjects when used alone: however, this should not be dependent on a decrease in gonadotropins.
Now let’s look at some other effects not necessarily related to the androgenicity of foods .
Between this we remember:Let’s pause for a moment to think about the side effects, which are arguably the worst of the short term. Sexuals do you think they are an advantage.
We say yes, but I must remember that an increase in libido, if it is not satisfied (Freud teaches …), can be transformed into other types of drives, up to crime. Finally, remember that an initial increase inevitably follows a decrease after suspension for the physiological reasons explained above. When it comes to the impact on aggression, I remember that they often wish bodybuilders or powerlifters to go to the gym more busy to lift huge weights. I do not deny that it is effective, but at what cost! If you really feel like you need the extra nerve to gain weight, it can mean many things, for example:- You are probably mildly overtrained or the routine is boring and unproductive;
- You have other psychological problems;
- You are not made for this sport;
- In all the above cases, you are still wrong.
Dealing with these anabolic psychological “disorders” is absurd; It is better to act at the root of the problem, eliminate harmful causes and learn to control your mind, how to control your muscles. There are special methods for all this (self-hypnosis, autogenous training). As for other anabolic steroids, it should be said that their effect on libido and aggression seems to be related to the degree of androgenicity: from my own experience, I have even seen that few androgenic products (e.g. winstrol) tend to even decrease libido in some subjects when used alone: however, this should not be dependent on a decrease in gonadotropins.
Now let’s look at some other effects, not necessarily related to the androgenicity of foods. These include:
- Altered blood sugar … Androgenic anabolic agents can increase insulin sensitivity, this usually does not lead to hypoglycemia, but to a possible increase in its effects, that is, increase in fat, water retention, etc. These phenomena seem to be more pronounced in drugs that are sensitive to peripheral aromatization.
- Modification of blood lipids (fats) . I will dwell on this aspect for a moment, among the latter to be discovered. Androgenic-anabolic substances tend to reduce triglyceride levels by reducing the concentration of very low density lipoproteins (VLDL): this effect, in itself positive, is inherent in some derivatives of the progestogen nortestosterone, partly the same durabolin, oxandrolone, etc. However, over the past 5 years, they have been found to dramatically lower high-density lipoprotein levels, which carry the “good” portion of cholesterol (that is, HDL, which is the one that clears the arteries), and instead raise cholesterol levels associated with LDL lipoproteins (which Clog the arteries, predisposing to atherosclerosis).
And think that they were even used to treat hypertriglyceridemia! The effect does not depend on the dose, but, by blocking a certain enzymatic pathway, it appears already in small doses, and sometimes within just 2 days. All drugs, regardless of their characteristics (androgenicity, aromatization), seem to share it. Now, this side effect (along with the hypertension, which I will continue about) is the most dangerous mean to me. Not noticing that nothing (while acne and water retention become clearly visible), the arteries become blocked.It cannot be said that atherosclerosis affects all those who take anabolic drugs, but there is no doubt that the risk increases enormously, and not in a probabilistic way ( such as smoking – lung cancer), but much more direct, that is, associated with the duration of… What is usually the first sign of atherosclerosis in a relatively young subject? It is easy to say: death from a heart attack. In the following years, the manifestations, although very serious, become more treatable (with medication, surgery, etc.), but I think you all know what it means to suffer from the heart. Other complications occur at an older age (60-70 years) on the kidneys, brain, etc. Therefore, please do not say that “those who take anabolic are healthy like fish” or something like that: it seems as healthy as a fish, but his arteries are very likely to be destroyed, and would be curious to know if in middle age, especially when you stop exercising, I still feel so good.
Tendency to water retention and hypertension . This side effect is partly dependent on estrogen, but also on the androgen effect itself and / or on the effect on insulin (see above) or endogenous cortisone, all hormones that cause water retention. Water retention in the uninitiated is manifested by edema, especially on the face, ankles; then the bodybuilder, who usually looks in the mirror, will notice the often conspicuous definition, even if the body fat remains the same, that is, it is “smoothed”. Water retention can be roughly measured with a balance: weight that increases rapidly (2-3 days) and disappears just as quickly when the drug is discontinued is nothing more than water retention.Obviously, the most androgenic and flavored foods (testosterone , dianabol, boldenone) are given almost always, even depending on the dose; much less androgenic (methandriol, especially deca) and even less non-aromatized androgens (winstrol, oxandrolone, primobolan)… Of course, it is common knowledge that the ease with which water is retained, even with equal doses of the same drug, varies greatly from person to person, as do all side effects in general: as a rule, people with a tendency to slow metabolism retain more water, probably because Under these conditions, the transformation of steroids is more focused on the production of estrogen (through metabolic 5-beta reduction) than other products (through 5-alpha), and also because the metabolism of cortisol itself is slowed down. Finally, in the same person, the delay is much more apparent with a free diet (carbohydrates) than with a very limited diet. In some cases, retention does not present any other obvious problem besides aesthetic; in others, it is accompanied by an increase in blood pressure. In young and healthy people, the increase in pressure can only be temporary (for several days), because later the mechanisms of self-regulation, as a rule, return it to its place; but in some cases the pressure remains high. Therefore, it is almost imperative that every good gym has a sphygmomanometer, perhaps an automatic type, so that all those who do weight (anabolic or not) can check themselves regularly. Remember that those with very large hands may have falsely higher values of 10-15 mmHg. Art.
Gynecomastia . This means the appearance, to a large extent, of tissue similar to a woman’s breasts in the area behind the nipple. This phenomenon is easily distinguishable from “boobs” in obese males (when the swelling occurs from adipose tissue, and not from the mammary glands), this phenomenon is observed physiologically almost in half of the adolescents, and then disappears. This is naturally due to estrogen. Highly androgenic and aromatized steroids (as well as a diuretic commonly used by bodybuilders, spironolactone or aldactone) can also cause it in adults if taken in excessive doses for extended periods of time… If you allow it to develop, this defect, often even painful, will unfortunately become irreversible (surgery is required).
Liver toxicity . In the past, this has been the most famous side effect of anabolic steroids. In fact, testosterone itself is not toxic to the liver at all, on the contrary, it helps limit the damage it undergoes from numerous toxic substances (alcohol, etc.), so much so that it was once used as an adjuvant in the treatment of liver cirrhosis … The same goes for derivatives. The toxicity attributed to steroids does not depend on the fact that they are steroids, but on the molecular change (alkylation at the 17-alpha position) that many of them have, that is, “traditional” oral. Some injectable drugs are also 17-alpha alkylated (winstrol, methandriol), which is a controversy because alkylation is necessary to prolong the life of orally administered drugs in the body (otherwise the liver will eliminate them immediately). The toxicity of alkylates, as always, depends on time and dose. The first signs consist of inflammation of the bile ducts with jaundice, at first not obvious, and then clinical (the sclera, that is, the white parts of the eyes, are the first areas where jaundice is observed), then an increase in the level of Gamma Gt in the blood. then SGOT and finally SGPT. Many malignant liver tumors (hepatomas) have been attributed to the use of these products, unfortunately, also in bodybuilders.Of course, those who want to check their luggage will say that the tests are not definitive, but in the face of even one similar risk I would say that both it is probably best to avoid taking alkylates that have similar or identical non-toxic liver products.
Finally, another effect of anabolic agents has been attributed to 17-alpha-alkylation, namely the anticoagulant effect… In fact, due to increased fibrinolysis (i.e., the clot is easier to remove), this phenomenon is also observed with non-alkylated products such as ethylestrenol and nandrolones (deca-durabolin). Unless the person has had preexisting coagulation changes, this effect is relatively harmless.
What are the therapeutic indications for these drugs?
Their androgenic characteristics are mainly used to maintain or develop sexual characteristics in cases of deficiency; anabolic performance in case of protein depletion. But let’s see what is mainly used:- In case of infertility due to azoospermia (i.e. a decrease in sperm count).
- Conditions of low sexual potency (even if due to psychological reasons) can be treated with androgens (typically up to 200 mg / week) given their well-documented role in libido development and maintenance.
- In some cases of breast cancer in women, they are used to curb (unfortunately only palliatively) the development of cancer and pain, in this case, non-aromatized androgens are preferably used in doses that must necessarily be higher than in men: subsequent virilization tolerable given the severity of the disease.
- Anabolic agents have instead been used in cases of protein malnutrition in adults and incorrectly in children (see the case of Dianabol). They improve appetite and, together with proper nutrition, stimulate protein synthesis.
- Similarly, they are used in certain preoperative conditions to improve the trophism of the patient due to severe stress or after the operation itself to facilitate recovery during the recovery period; for the same reason they have been used in severely injured patients or, more generally, in patients forced to lie in bed for extended periods of time to reduce protein catabolism due to stress and / or non-use.
- They are used for severe burns to stimulate faster repair of damaged tissue.
- They are now widely used in the treatment of osteoporosis in both sexes to stimulate bone protein matrix formation and calcium deposition.
- They are often associated with cortisone drugs in chronic therapy to minimize the catabolic effects of these drugs (highly visible on bone, muscle, skin, etc.).
- They are also sometimes used in cases of arthritis or arthrosis and other chronic conditions.
- Finally, for aplastic anemias (that is, those not associated with vitamin B12 or folic acid deficiencies), they were used in very strong doses (before testosterone was used, then we switched to an anabolic drug such as decadurabolin, so as it was seen that the effectiveness was the same, with fewer side effects).
Obviously the average athlete doesn’t get into any of these cases (hopefully); why then do you use anabolic steroids?
Through their use we are trying to stimulate protein synthesis to increase muscle mass and strength, or in resistance to prolonged effort in middle distance athletes. However, the scientific community has not yet been able to demonstrate the effectiveness of these drugs as ergogenic, due in part to the stringency of criteria commonly used in research protocols. Many authors believe that every beneficial effect attributed to steroids is in fact related to the so-called “effect placebo ”(that is, to believe that the substance is good, followed by an improvement in training, etc., in the particular case of the athlete). .
I will cite two of the best studies in this area:- Fowler et al. in a double-blind study (neither they nor the athletes knew who was taking the placebo or who was taking the drug) tested 47 students aged 28 to 25… 10 were footballers, so athletes trained, the rest were not. Six groups were made (players with half placebos and half drugs, sedentary or not, drug or placebo). Androstenolone was used at a dose of 20 mg per day for 16 weeks. Neither group experienced significant increases in weight, strength, or muscle mass.
- Casner et al conducted a 1971 study on the effect of Winstrol on 27 college students. There were also 4 groups made here: students with placebo or drugs and with or without (resistance) training. Among the parameters measured was a significant increase in body weight in those taking Winstrol, which means that they gained more weight than the placebo. Further analysis, however, appears to make it clear that the weight gain was associated with water retention and not with actual gains in muscle mass. Even here, according to the authors, there was no reason for the use of anabolic steroids in athletes.
HOW TO MINIMIZE SIDE EFFECTS
Unfortunately, those who have decided to take or are already taking anabolic medications will not (I’m afraid) be convinced or intimidated by the above. Although, of course, I do not recommend taking these substances from a medical point of view for the sole purpose of improving athletic performance, of course, many will continue to take them. And therefore it must be said for them that it is also true that, like any other medicine, the frequency of side effects can truly be minimized if the bodybuilder uses steroids correctly. And let’s see how.
Of course, the dose used is a critical factor: let’s explain why with a few small pharmacology notes.
Each drug has the desired action (main effect). At a certain “threshold” dose, nothing happens. Above this dose, the effect manifests itself and increases with increasing dose in an indirect way (i.e…. does not triple when the dose is tripled), but is usually logarithmic. Upon reaching a certain dose, the effect no longer increases, if not insignificantly (property of logarithms), even at doses tens of times higher. Various side effects also have a “range” of reaction, often different from the main effect.Let’s take testosterone as an example.
Less than 15 mg / week, each effect is minimal. Already at 35 mg / week, a clear nitrogen retention effect is observed. There is no water retention or marked inhibition of gonadotropins at these doses (side effects). By gradually increasing the dose, we will have from 40 to 200 mg per week, first partial and then complete inhibition of gonadotropins. The nitrogen retention effect reaches almost maximum at 200 mg / week, the well-known effect is only twice as high as with a 5-fold reduced dose.
At 400 mg / week, nitrogen retention no longer increases and instead it is clear that water one.
Finally, at doses over 1000 mg (once used to treat certain anemias), virilization and retention are intrusive.
Thus, careful use of a drug that plays at doses already makes a difference.Another factor related to dose size is the length of the dose period. The discussion is similar to the previous one, Each effect takes its own time.
Water and salt retention is a rather fast process (2-3 days), carbohydrates and potassium are slower, phosphorus is slower (months) and nitrogen is bound to even slower contractile proteins. Inhibition of spermatogenesis is completed in 3-5 months. Then “virilization” (apparently in children and women) occurs very slowly and, as you know, ends in years, not months. The concept of reversibility is also related to duration of action. Virilization is known to be almost irreversible; atherosclerosis is very small if caught early.It follows from all this that medications, as a rule, should be taken in the shortest possible time necessary for building muscle proteins. Experience shows that a good anabolic effect is achieved after 4-6 weeks: at these doses, testicular atrophy and serum lipid modification are rather scarce.
The concept of dose is perhaps even more important in the case of low androgenic anabolic substances, which, as mentioned at the beginning are usually true at low doses. and they become more androgenic at higher doses. Using steroids that are too high and causing more side effects will only increase your risk of becoming “insensitive” to the drug itself. This phenomenon, typical of endocrinology, may be due to the fact that the cellular structures responsible for recognizing steroids and receiving the message of war (receptors) decrease in number if they are exposed for a long time to too high concentrations of the same, as to protect cells from overdose.
This phenomenon is called down-regulation (sub-regulation) and is also typical of thyroid hormones (beware !!!), insulin and other hormones ..
Well, many so-called drug formulators believe that switching from one steroid to another is a method of eliminating downregulation.
You won’t believe that mother nature has created as many different types of receptors as there are steroids. on the market! There is only one steroid receptor, and if it decreases, the effect of any anabolic steroid will decrease. It also follows how wrong another typical bodybuilding practice is: stacking (using two or more steroids together) or even “bombarding” (megadoses of different drugs, type 100 deca, 200 testosterone, 200 primobolan … per day!): If the receptor ( poor guy) only one, you only put it in your underwear.
Rather, it must be said that just because the receptor is the same does not mean that different foods have the same effect. In fact, once inside the cell, the steroid can be metabolized in different ways (I mentioned this earlier), causing different effects: c. for example, a more noticeable increase in phosphocreatine and mitochondria for a more androgenic (“massive” effect), a more noticeable increase in contractile proteins for a less androgenic (“power” effect), etc.
I advise you to re-read well what I wrote and keep this in mind. During steroid therapy (and even after its termination) it would be good to check at least the following indicators:- pressure once a week
- Body weight every day (an increase of more than 1 kg per week is an undeniable indicator of water retention)
- A in the blood – SGOT, SGPT, Gamma-Gt, bilirubins, total cholesterol, triglycerides and HDL cholesterol (or protein electrophoresis).
- Every 3-6 months, especially if you are under strong androgen, you should have a rectal exam.
It is not advisable to bring these tests to your doctor, unless he is an expert in the field and is not friendly with you, Seek a doctor who knows the environment and whom you trust to help you interpret the tests in light the fact that you are taking steroids.
If, at last, side effects appear, what to do? I have to say this on an individual basis. However, in general I would say:
- If liver enzymes (SGOT, SGPT, Gamma-Gt or Bilirubin) change, stop using 17-alpha alkylates (Winstrol, Oxandrolon abnehmen, Dianabol, etc.) and forget about them for the rest of your life. If you didn’t take them instead, it’s very likely that you have real liver disease, regardless of steroids..
- If you have a tendency to have low HDL cholesterol levels even in normal conditions and / or family members (dad, uncle, grandparents) with a history of heart attack, check this index very carefully and, if you really need to, do short cycles. Then try (but that’s even if you’re not on steroids) regularly aerobics throughout your life (that’s not what I’m talking about in terms of sports prevention, I’m not talking here).
- In case of acne, avoid ignoring it until you become a leper. Miracles don’t work here, just: a) avoid using highly androgenic products and do not exceed therapeutic doses b) cleanse your skin properly and use antibiotic ointments (although acne, although androgens prefer them, is a bacterial infection) c) try to stay in the sun if it is possible.
- In the case of gynecomastia, you will almost always find testosterone or dianabol responsible. Well, all you have to do is stop them and you won’t have to take any more flavored drugs.
- In the event of excessive (for your usual purposes) water retention, reduce the doses and you will see this phenomenon almost always subside. If this continues, be aware that there are other ways to reduce water retention, many of which are possibly worse than water retention ..
One more article is required for their exhaustive consideration, so I will only mention:
- Diuretics : they deplete salts, the effect is often uncontrollable, and if you really need to, use them for several days (and with appropriate supplementation) of minerals, which is strictly dependent on the diuretic or combinations of diuretics used). They can be very dangerous (if not for life, of course for a sports presentation: consider doing weight or doing cramps racing …)… However, diuretics were recently banned from IFBB racing.
- Antiestrogens : (tamoxifen or nolvadex, testonolactone and testolac, cyclophenyl). They are quite toxic drugs in the long run; they tend to give a slurry rebound effect (that is, when you stop them, you swell like balls), and this only acts on the estrogenic component of water retention anyway. Better not to use them at all. Their use can only be reserved for those who (often, even if they do not take anything) have really high estrogen levels (above 40 pg / ml, as confirmed by a blood test that still takes it) and suffer from delay
- Diet Monitoring . Of course, if you limit the amount of carbohydrates, the delay disappears, but it doesn’t make sense if you are in the mass phase. Better to limit your sodium intake with a computerized diet: I say, limit, don’t rule out, because if you eat too little you will lose potassium, and even then you will have a blessed rebound (due to overproduction of the sodium-friendly hormone aldosterone ) and you would be very bloated like frogs if you eat food rich in salt. Instead of salt, limiting water intake, which is more than dangerous, is completely useless (the body sets up systems to retain even the small amount that you must take).
Finally, among natural systems, the most effective and beneficial is undoubtedly the regular practice of aerobic activities, such as running or cycling, which, unfortunately, almost no one does. Those who tend to suffer from retention should gradually engage in aerobics (not dance!) And stay in training… It is not true that running makes you lose muscle; it only does so if, due to too low aerobic fitness (where you are, of course, if you are doing weights only), you increase your running doses too quickly.
And the last, the last word for women: I leave aside the debate about whether women should be muscular or rather flexible and slim (soft, tough, etc.). From a purely medical point of view, a woman who really wants to take an anabolic should definitely do it under the strict supervision of a specialist doctor (endocrinologist), since ultimately these are male hormones. In addition to the side effects associated with more or less pronounced masculinization, there is a risk of damage to all female functions (menstruation, possibility of pregnancy) due to their very delicate nature.
Read more about this article
I liked this article primarily because it focuses on aspects of AAS danger that are usually ignored: we usually only deal with the axis, pituitary, gynuids and liver. But no one has ever died of hypogonadism, and even cases of liver tumors are indeed rare and statistically insignificant. Instead, it’s clear that premature deaths from heart attacks are more common in bodybuilders…. The fact that bomber jackets are the least affected by cancer in the US population does not permit myocardial suicide.However, to make prevention as effective as possible, it is good to be as precise as possible, so two more words on how negative is expressed. the effect of AAS on lipids; is an effect that, in addition to being dose dependent, is formulated differently according to certain characteristics of the AAS:
- alkylates show the ability to worsen the HDL / LDL ratio at any dosage, even if they sometimes lower total cholesterol (especially oxandrolone and furazabol);
- unalkylated, on the other hand, exhibit this effect only at various high doses, depending on the specific substance, with non-flavorants, which exhibit this attitude at lower doses than with flavored; even fragrances have the paradoxical effect of improving lipids at the lowest doses.
For example, testosterone enanthate at a dose of 100 mg per week shows a clear lipid-enhancing effect, which, although decreasing, still remains at 300 mg; at 600 mg it leaves them unchanged, and at 900 the negative effect is evident. Probably, in men suffering from hypogonadism, this data will have to be slightly retouched upwards. For the prostate, I would be less alarmist: it is now established that benign hypertrophy is caused by estrogens and progestins, while for malignant there is no evidence of a connection with androgens: the experiment that started this dogma was from 1941 and is completely unreliable for the methods of execution and also for the partial report to which he was subject. For women, the discussion goes against the usual discussion in men of not only fertility loss, which is sometimes welcome, but also the specific dependence of female hormones, as well as the positive effects that AAS can have…. in counteracting those psycho-nutritional disorders that women are more likely to experience
Let’s pause for a moment to think about the side effects, which are arguably the worst of the short term. As for the sexual ones, you think they are an advantage.
We say yes, but I must remember that an increase in libido, if not satisfied (Freud teaches …), can transform into other types of drives, up to before the crime. Finally, remember that an initial increase inevitably follows a decrease after suspension for the physiological reasons explained above. When it comes to the impact on aggression, I remember that they often wish bodybuilders or powerlifters to go to the gym more busy to lift huge weights. I do not deny that it is effective, but at what cost! If you really feel like you need the extra nerve to gain weight, it can mean many things, for example:- You are probably mildly overtrained or the routine is boring and unproductive;
- You have other psychological problems;
- You are not made for this sport;
- In all the above cases, you are still wrong.
Dealing with these anabolic psychological “disorders” is absurd; It is better to act at the root of the problem, eliminate harmful causes and learn to control your mind, how to control your muscles. There are special methods for all this (self-hypnosis, autogenous training). As for other anabolic steroids, it should be said that their effect on libido and aggression seems to be related to the degree of androgenicity: from my own experience, I have even seen that few androgenic products (such as winstrol) in some subjects there is a tendency to decrease even libido if used alone: however, this should not be dependent on a decrease in gonadotropins.
Now let’s look at some other effects, not necessarily related to the androgenicity of foods. These include:- Altered blood sugar . Androgenic anabolic agents can increase insulin sensitivity, this usually does not lead to hypoglycemia, but to a possible increase in its effects, that is, increase in fat, water retention, etc. These phenomena seem to be more pronounced in drugs that are sensitive to peripheral aromatization.
- Modification of blood lipids (fats) . I will dwell on this aspect for a moment, among the latter to be discovered. Androgenic-anabolic substances tend to reduce triglyceride levels by reducing the concentration of very low density lipoproteins (VLDL): this effect, in itself positive, is inherent in some derivatives of the progestogen nortestosterone, partly the same durabolin, oxandrolone, etc. However, over the past 5 years, they have been found to dramatically lower high-density lipoprotein levels, which carry the “good” portion of cholesterol (that is, HDL, which is the one that clears the arteries), and instead raise cholesterol levels associated with LDL lipoproteins (which “Pollute” the arteries, causing a predisposition to atherosclerosis). And think that they were even used to treat hypertriglyceridemia! The effect does not depend on the dose, but, by blocking a certain enzymatic pathway, it appears already in small doses, and sometimes within just 2 days. All drugs, regardless of their characteristics (androgenicity, aromatization), seem to share it. Now, this side effect (along with the hypertension, which I will continue about) is for me the most dangerous vile… Without noticing that nothing (while acne and water retention become clearly visible), the arteries become blocked, It cannot be said that atherosclerosis affects all those who take anabolic drugs, but it is undoubted that the risk increases enormously, and not in a probabilistic way ( such as smoking – lung cancer), but much more direct, that is, associated with the duration of intake. What is usually the first sign of atherosclerosis in a relatively young subject? It is easy to say: death from a heart attack. In the following years, the manifestations, although very serious, become more treatable (with medication, surgery, etc.), but I think you all know what it means to suffer from the heart. Other complications occur at an older age (60-70 years) on the kidneys, brain, etc. Therefore, please do not say that “those who take anabolic are healthy as fish” or something like that: it seems healthy as a fish, but his arteries are very likely to be destroyed, and would be curious to know if middle age, especially when you stop exercising, still feel so good.
- Tendency to water retention and hypertension . This side effect is partly dependent on estrogen, but also on the androgen effect itself and / or on the effect on insulin (see above) or endogenous cortisone, all hormones that cause water retention. Water retention in the uninitiated is manifested by edema, especially on the face, ankles; then the bodybuilder, who usually looks in the mirror, will notice the often conspicuous definition, even if the body fat remains the same, that is, it is “smoothed”… Water retention can be roughly measured with a balance: weight that increases rapidly (2-3 days) and disappears just as quickly when the drug is discontinued is nothing more than water retention.Obviously, the most androgenic and flavored foods (testosterone , dianabol, boldenone) are given almost always, even depending on the dose; much less small androgens (methandriol, especially deca) and even less small non-aromatized androgens (winstrol, oxandrolone, primobolan). Of course, it is common knowledge that the ease with which water is retained, even with equal doses of the same drug, varies greatly from person to person, as do all side effects in general: as a rule, people with a tendency to slow metabolism retain more water, probably because Under these conditions, the transformation of steroids is more focused on the production of estrogen (through metabolic 5-beta reduction) than other products (through 5-alpha), and also because the metabolism of cortisol itself is slowed down. Finally, in the same person, the delay is much more apparent with a free diet (carbohydrates) than with a very limited diet. In some cases, retention does not present any other obvious problem besides aesthetic; in others, it is accompanied by an increase in blood pressure. In young and healthy people, the increase in pressure can only be temporary (for several days), because later the mechanisms of self-regulation, as a rule, return it to its place; but in some cases the pressure remains high. Therefore, it is almost imperative that every good gym has a sphygmomanometer, perhaps an automatic type, so that all those who do weight (anabolic or not) can check themselves regularly. Remember that those with very large hands may have falsely higher values of 10-15 mm / Hg. Art.
- gynecomastia … This means the appearance, to a large extent, of tissue similar to a woman’s breasts in the area behind the nipple. This phenomenon is easily distinguishable from “boobs” in obese males (when the swelling occurs from adipose tissue, and not from the mammary glands), this phenomenon is observed physiologically almost in half of the adolescents, and then disappears. This is naturally due to estrogen. Highly androgenic and aromatized steroids (as well as a diuretic commonly used by bodybuilders, spironolactone or aldactone) can also cause it in adults if taken in excessive doses for extended periods of time. If you allow it to develop, this defect, often even painful, unfortunately, will become irreversible (surgery is required).
- Liver toxicity . In the past, this has been the most famous side effect of anabolic steroids. In fact, testosterone itself is not toxic to the liver at all, on the contrary, it helps limit the damage it undergoes from numerous toxic substances (alcohol, etc.), so much so that it was once used as an adjuvant in the treatment of liver cirrhosis … The same goes for derivatives. The toxicity attributed to steroids does not depend on the fact that they are steroids, but on the molecular change (alkylation at the 17-alpha position) that many of them have, that is, “traditional” oral. Some injectable drugs are also 17-alpha alkylated (winstrol, methandriol), which is a controversy because alkylation is necessary to prolong the life of orally administered drugs in the body (otherwise the liver will eliminate them immediately). The toxicity of alkylates, as always, depends on time and dose. The first signs consist of inflammation of the bile ducts with jaundice, at first not obvious, and then clinical (the sclera, that is, the white parts of the eyes, are the first areas where jaundice is observed), then an increase in the level of Gamma Gt in the blood. then SGOT and finally SGPT… Many malignant liver tumors (hepatomas) have been attributed to the use of these products, unfortunately, also in bodybuilders.Of course, those who want to check their luggage will say that the tests are not definitive, but in the face of even such a risk I would say that how can rather, it is best to avoid taking alkylates that have similar or identical non-toxic liver products.
Finally, another effect of anabolic agents has been attributed to 17-alpha-alkylation, namely the anticoagulant effect. In fact, due to increased fibrinolysis (i.e., the clot is easier to remove), this phenomenon is also observed with non-alkylated products such as ethylestrenol and nandrolones (deca-durabolin). Unless the person has had any pre-existing coagulation changes, this effect is relatively harmless.
What are the therapeutic indications for these drugs?
Their androgenic characteristics are mainly used to maintain or develop sexual characteristics in cases of deficiency; anabolic performance in case of protein depletion. But let’s see what is mainly used:- In case of infertility due to azoospermia (i.e. a decrease in sperm count).
- Conditions of low sexual potency (even if due to psychological reasons) can be treated with androgens (usually up to 200 mg / week) given their well-documented role in the development and maintenance of libido.
- In some cases of breast cancer in women, they are used to curb (unfortunately only palliatively) the development of cancer and pain, in this case, non-aromatized androgens are preferably used in doses that must necessarily be higher than in men: subsequent virilization tolerable given the severity of the disease.
- Anabolic agents have instead been used in cases of protein malnutrition in adults and incorrectly in children (see… the case of Dianabol), They improve appetite and, together with proper nutrition, stimulate protein synthesis.
- Similarly, they are used in certain preoperative conditions to improve the trophism of the patient due to severe stress or after the operation itself to facilitate recovery during the recovery period; for the same reason they have been used in severely injured patients or more generally in patients who have to lie in bed for extended periods of time to reduce protein catabolism due to stress and / or disuse.
- They are used for severe burns to stimulate faster repair of damaged tissue.
- They are now widely used in the treatment of osteoporosis in both sexes to stimulate bone protein matrix formation and calcium deposition.
- They are often associated with cortisone drugs in chronic therapy to minimize the catabolic effects of these drugs (highly visible on bone, muscle, skin, etc.).
- They are also sometimes used in cases of arthritis or arthrosis and other chronic conditions.
- Finally, for aplastic anemias (that is, those not associated with vitamin B12 or folic acid deficiencies), they were used in very strong doses (before testosterone was used, then we switched to an anabolic drug such as decadurabolin, so as it was seen that the effectiveness was the same, with fewer side effects).
Obviously the average athlete doesn’t get into any of these cases (hopefully); why then do you use anabolic steroids?
Through their use we are trying to stimulate protein synthesis to increase muscle mass and strength, or resistance to prolonged effort in middle distance athletes… However, the scientific community has not yet been able to demonstrate the effectiveness of these drugs as ergogenic, due in part to the stringency of criteria commonly used in research protocols. Many authors believe that every beneficial effect attributed to steroids is in fact related to the so-called “effect placebo ”(that is, to believe that the substance is good, followed by an improvement in training, etc., in the particular case of the athlete). .
I will cite two of the best studies in this area:- Fowler et al. in a double-blind study (neither they nor the athletes knew who was taking the placebo or who was taking the drug) tested 47 students between the ages of 28 and 25. 10 were footballers, so athletes trained, the rest were not. Six groups were made (players with half placebos and half drugs, sedentary or not, drug or placebo). Androstenolone was used at a dose of 20 mg per day for 16 weeks. Neither group experienced significant increases in weight, strength, or muscle mass.
- Casner et al conducted a 1971 study on the effect of Winstrol on 27 college students. There were also 4 groups made here: students with placebo or drugs and with or without (resistance) training. Among the parameters measured was a significant increase in body weight in those taking Winstrol, which means that they gained more weight than the placebo. Further analysis, however, appears to make it clear that the weight gain was associated with water retention and not with actual gains in muscle mass. Even here, according to the authors, there was no reason for the use of anabolic steroids in athletes.
HOW TO MINIMIZE SIDE EFFECTS
Unfortunately, those who have decided to take or are already taking anabolic medications will not (I am afraid) be convinced or afraid of the above… Although, of course, I do not recommend taking these substances from a medical point of view for the sole purpose of improving athletic performance, of course, many will continue to take them. And therefore it must be said for them that it is also true that, like any other medicine, the frequency of side effects can truly be minimized if the bodybuilder uses steroids correctly. And let’s see how.
Of course, the dose used is a critical factor: let’s explain why with a few small pharmacology notes.
Each drug has the desired action (main effect). At a certain “threshold” dose, nothing happens. Above this dose, the effect manifests itself and increases with increasing dose indirectly (i.e., it does not triple when the dose is threefold), but is usually logarithmic. Upon reaching a certain dose, the effect no longer increases, if not insignificantly (property of logarithms), even at doses tens of times higher. Various side effects also have a “range” of reaction, often different from the main effect.Let’s take testosterone as an example.
Less than 15 mg / week, each effect is minimal. Already at 35 mg / week, a clear nitrogen retention effect is observed. There is no water retention or marked inhibition of gonadotropins at these doses (side effects). By gradually increasing the dose, we will have from 40 to 200 mg per week, first partial and then complete inhibition of gonadotropins. The nitrogen retention effect reaches almost maximum at 200 mg / week, the well-known effect is only twice as high as with a 5-fold reduced dose.
At 400 mg / week, nitrogen retention no longer increases and instead it is clear that water one.
Finally, in doses greater than 1000 mg (once used to treat some anemias), virilization and retention is imposed. difference.Another factor related to dose size is the length of the dose period… The discussion is similar to the previous one, Each effect takes its own time.
Water and salt retention is a rather fast process (2-3 days), carbohydrates and potassium are slower, phosphorus is slower (months) and nitrogen is bound to even slower contractile proteins. Inhibition of spermatogenesis is completed in 3-5 months. Then “virilization” (apparently in children and women) occurs very slowly and, as you know, ends in years, not months. The concept of reversibility is also related to duration of action. Virilization is known to be almost irreversible; atherosclerosis is very small if caught early.It follows from all this that medications, as a rule, should be taken in the shortest possible time necessary for building muscle proteins. Experience shows that a good anabolic effect is achieved after 4-6 weeks: at these doses, testicular atrophy and serum lipid modification are rather scarce.
The concept of dose is perhaps even more important in the case of low androgenic anabolic substances, which, as mentioned at the beginning are usually true at low doses. and they become more androgenic at higher doses. Using steroids that are too high and causing more side effects will only increase your risk of becoming “insensitive” to the drug itself. This phenomenon, typical of endocrinology, may be due to the fact that the cellular structures responsible for recognizing steroids and receiving the message of war (receptors) decrease in quantity if they are exposed for a long time to too high concentrations of the same, as to protect the cell from overdose.
This phenomenon is called down-regulation (sub-regulation) and is also typical of thyroid hormones (beware !!!), insulin and other hormones ..
Well, many so-called formulators believe that switching from one steroid to another is a method of eliminating downregulation.
You won’t believe that mother nature has created as many different types of receptors as steroids. on the market! There is only one steroid receptor, and if it decreases, the effect of any anabolic steroid will decrease. It also follows how wrong another typical bodybuilding practice is: stacking (using two or more steroids together) or even “bombarding” (megadoses of different drugs, type 100 deca, 200 testosterone, 200 primobolan … per day!): If the receptor ( poor fellow) only one, you put it only in your underwear.
Rather, it must be said that if the receptor is the same, this does not mean that different products have the same effect. In fact, once inside the cell, the steroid can be metabolized in different ways (I mentioned this earlier), causing different effects: c. for example, a more noticeable increase in phosphocreatine and mitochondria for a more androgenic (“massive” effect), a more noticeable increase in contractile proteins for a less androgenic (“power” effect), etc.
I advise you to re-read well what I wrote and keep this in mind. During steroid therapy (and even after its termination) it would be good to check at least the following indicators:- pressure once a week
- Body weight every day (an increase of more than 1 kg per week is an undeniable indicator of water retention)
- A in the blood – SGOT, SGPT, Gamma-Gt, bilirubins, total cholesterol, triglycerides and HDL cholesterol (or protein electrophoresis).
- Every 3-6 months, especially if you are under strong androgen, you should have a rectal exam.
It is not advisable to bring these tests to your doctor, unless he is an expert in the field and is not friendly with you, Seek a doctor who knows the environment and whom you trust to help you interpret the tests in light the fact that you are taking steroids.
If, at last, side effects appear, what to do? I have to say this on an individual basis. However, in general I would say:
- If liver enzymes (SGOT, SGPT, Gamma-Gt or Bilirubin) change, stop using 17-alpha alkylates (Winstrol, Oxandrolone, Dianabol, etc.) and forget about them for the rest of your life. If you didn’t take them instead, it’s very likely that you have real liver disease, regardless of steroids.
- If you have a tendency to have low HDL cholesterol levels even in normal conditions and / or family members (dad, uncle, grandparents) with a history of heart attack, check this index very carefully and, if you really need to, do short cycles. Then try (but that’s even if you’re not on steroids) regularly aerobics throughout your life (that’s not what I’m talking about in terms of sports prevention, I’m not talking here).
- In the event of acne, avoid ignoring it until you become a leper. Miracles don’t work here, just: a) avoid using highly androgenic products and do not exceed therapeutic doses b) cleanse your skin properly and use antibiotic ointments (although acne, although androgens prefer them, is a bacterial infection) c) try to stay in the sun if it is possible.
- In the case of gynecomastia, you will almost always find testosterone or dianabol responsible. Well, all you can do is stop them and you won’t have to take any more flavored drugs.
- In the event of excessive (for your usual purposes) water retention, reduce the doses and you will see this phenomenon almost always subside. If this continues, be aware that there are other ways to reduce water retention, many of which are arguably worse than having it..
One more article is required for their exhaustive consideration, so I will only mention:
- Diuretics : they deplete salts, the effect is often uncontrollable, and if you really need to, use them for several days (and with appropriate supplementation) of minerals, which is strictly dependent on the diuretic or combinations of diuretics used). They can be very dangerous (if not for life, of course, for a sports presentation: consider doing weight or doing cramps racing …). However, diuretics were recently banned from IFBB racing.
- Antiestrogens : (tamoxifen or nolvadex, testonolactone and testolac, cyclophenyl). They are quite toxic drugs in the long run; they tend to give a slurry rebound effect (that is, when you stop them, you swell like balls), and this only acts on the estrogenic component of water retention anyway. Better not to use them at all. Their use can only be reserved for those who (often, even if they do not take anything) have really high estrogen levels (above 40 pg / ml, as confirmed by a blood test that still takes it) and suffer from delay
- Diet Monitoring . Of course, if you limit the amount of carbohydrates, the delay disappears, but it doesn’t make sense if you are in the mass phase. Better to limit your sodium intake with a computerized diet: I say, limit, don’t rule out, because if you eat too little you will lose potassium, and even then you will have a blessed rebound (due to overproduction of the sodium-friendly hormone aldosterone ) and you would be very bloated like frogs if you eat food rich in salt… Instead of salt, limiting water intake, which is more than dangerous, is completely useless (the body sets up systems to retain even the small amount that you must take).
Finally, among natural systems, the most effective and beneficial is undoubtedly the regular practice of aerobic activities, such as running or cycling, which, unfortunately, almost no one does. Those who tend to suffer from retention should gradually practice aerobics (not dance!) And stay in training. It is not true that running makes you lose muscle; it only does so if, due to too low aerobic fitness (where you are, of course, if you are doing weights only), you increase your running doses too quickly.
And the last, the last word for women: I leave aside the debate about whether women should be muscular or rather flexible and slim (soft, tough, etc.). From a purely medical point of view, a woman who really wants to take an anabolic should definitely do it under the strict supervision of a specialist doctor (endocrinologist), since ultimately these are male hormones. In addition to the side effects associated with more or less pronounced masculinization, there is a risk of damage to all female functions (menstruation, possibility of pregnancy) due to their very delicate nature.
- gynecomastia. This means the appearance, to a large extent, of tissue similar to a woman’s breasts in the area behind the nipple. This phenomenon is easily distinguishable from “boobs” in obese males (when the swelling occurs from adipose tissue, and not from the mammary glands), this phenomenon is observed physiologically almost in half of the adolescents, and then disappears. This is naturally due to estrogen. Highly androgenic and aromatized steroids (as well as a diuretic commonly used by bodybuilders, spironolactone or aldactone) can also cause it in adults if taken in excessive doses for extended periods of time. If you allow it to develop, this defect, often even painful, unfortunately, will become irreversible (surgery is required).
- Liver toxicity. In the past, this has been the most famous side effect of anabolic steroids. In fact, testosterone itself is not toxic to the liver at all, on the contrary, it helps limit the damage it undergoes from numerous toxic substances (alcohol, etc.), so much so that it was once used as an adjuvant in the treatment of liver cirrhosis … The same goes for derivatives. The toxicity attributed to steroids does not depend on the fact that they are steroids, but on the molecular change (alkylation at the 17-alpha position) that many of them have, that is, “traditional” oral. Some injectable drugs are also 17-alpha alkylated (winstrol, methandriol), which is a controversy because alkylation is necessary to prolong the life of orally administered drugs in the body (otherwise the liver will eliminate them immediately). The toxicity of alkylates, as always, depends on time and dose. The first signs consist of inflammation of the bile ducts with jaundice, at first not obvious, and then clinical (the sclera, that is, the white parts of the eyes, are the first areas where jaundice is observed), then an increase in the level of Gamma Gt in the blood. then SGOT and finally SGPT. Many malignant liver tumors (hepatomas) have been attributed to the use of these products, unfortunately, also in bodybuilders.Of course, those who want to check their luggage will say that the tests are not definitive, but in the face of even such a risk I would say that how can rather, it is best to avoid taking alkylates that have similar or identical non-toxic liver products.
Finally, another effect of anabolic agents has been attributed to 17-alpha-alkylation, namely the anticoagulant effect. In fact, due to increased fibrinolysis (i.e., the clot is easier to remove), this phenomenon is also observed with non-alkylated products such as ethylestrenol and nandrolones (deca-durabolin). Unless the person has had any pre-existing coagulation changes, this effect is relatively harmless.
What are the therapeutic indications for these drugs?
Their androgenic characteristics are mainly used to maintain or develop sexual characteristics in cases of deficiency; anabolic performance in case of protein depletion. But let’s see what is mainly used:
- In case of infertility due to azoospermia (i.e. a decrease in sperm count).
- Conditions of low sexual potency (even if due to psychological reasons) can be treated with androgens (usually up to 200 mg / week) given their well-documented role in the development and maintenance of libido.
- In some cases of breast cancer in women, they are used to curb (unfortunately only palliatively) the development of cancer and pain, in this case, non-aromatized androgens are preferably used in doses that must necessarily be higher than in men: subsequent virilization tolerable given the severity of the disease.
- Anabolic agents have instead been used in cases of protein malnutrition in adults and incorrectly in children (see the case of Dianabol). They improve appetite and, together with proper nutrition, stimulate protein synthesis.
- Similarly, they are used in certain preoperative conditions to improve the trophism of the patient due to severe stress or after the operation itself to facilitate recovery during the recovery period; for the same reason they have been used in severely injured patients or more generally in patients who have to lie in bed for extended periods of time to reduce protein catabolism due to stress and / or disuse.
- They are used for severe burns to stimulate faster repair of damaged tissue.
- They are now widely used in the treatment of osteoporosis in both sexes to stimulate bone protein matrix formation and calcium deposition.
- They are often associated with cortisone drugs in chronic therapy to minimize the catabolic effects of these drugs (highly visible on bone, muscle, skin, etc.).
- They are also sometimes used in cases of arthritis or arthrosis and other chronic conditions.
- Finally, for aplastic anemias (that is, those not associated with vitamin B12 or folic acid deficiencies), they were used in very strong doses (before testosterone was used, then we switched to an anabolic drug such as decadurabolin, so as it was seen that the effectiveness was the same, with fewer side effects).
Obviously the average athlete doesn’t get into any of these cases (hopefully); why then do you use anabolics?
Through their use, we are trying to stimulate protein synthesis to increase muscle mass and strength, or resistance to sustained effort in mid-distance athletes. However, the scientific community has not yet been able to demonstrate the effectiveness of these drugs as ergogenic, due in part to the stringency of criteria commonly used in research protocols. Many authors believe that every beneficial effect attributed to steroids is in fact related to the so-called “effect placebo ”(that is, to believe that the substance is good, followed by an improvement in training, etc., in the particular case of the athlete). .
I will cite two of the best studies in this area:
- Fowler et al. in a double-blind study (neither they nor the athletes knew who was taking the placebo or who was taking the drug) tested 47 students between the ages of 28 and 25. 10 were footballers, so athletes trained, the rest were not. Six groups were made (players with half placebos and half drugs, sedentary or not, drug or placebo). Androstenolone was used at a dose of 20 mg per day for 16 weeks. Neither group experienced significant increases in weight, strength, or muscle mass.
- Casner et al conducted a 1971 study on the effect of Winstrol on 27 college students. There were also 4 groups made here: students with placebo or drugs and with or without (resistance) training. Among the parameters measured was a significant increase in body weight in those taking Winstrol, which means that they gained more weight than the placebo. Further analysis, however, appears to make it clear that the weight gain was associated with water retention and not with actual gains in muscle mass. Even here, according to the authors, there was no reason for the use of anabolic steroids in athletes.
HOW TO MINIMIZE SIDE EFFECTS
Unfortunately, those who have decided to take or are already taking anabolic drugs will not (I fear) be convinced or intimidated by the above. Although, of course, I do not recommend taking these substances from a medical point of view for the sole purpose of improving athletic performance, of course, many will continue to take them. And therefore it must be said for them that it is also true that, like any other medicine, the frequency of side effects can truly be minimized if the bodybuilder uses steroids correctly. And let’s see how.
Of course, the dose used is a critical factor: let’s explain why with a few small pharmacology notes.
Each drug has the desired action (main effect). At a certain “threshold” dose, nothing happens. Above this dose, the effect manifests itself and increases with increasing dose indirectly (i.e., it does not triple when the dose is threefold), but is usually logarithmic. Upon reaching a certain dose, the effect no longer increases, if not insignificantly (property of logarithms), even at doses tens of times higher. Various side effects also have a “range” of reaction, often different from the main effect.
Let’s take testosterone as an example.
Less than 15 mg / week, each effect is minimal. Already at 35 mg / week, a clear nitrogen retention effect is observed. There is no water retention or marked inhibition of gonadotropins at these doses (side effects). By gradually increasing the dose, we will have from 40 to 200 mg per week, first partial and then complete inhibition of gonadotropins. The nitrogen retention effect reaches almost maximum at 200 mg / week, the well-known effect is only twice as high as with a 5-fold reduced dose.
At 400 mg / week, nitrogen retention no longer increases and instead it is clear that water one.
Finally, in doses greater than 1000 mg (once used to treat some anemias), virilization and retention is imposed. difference.
Another factor related to dose size is the length of the dose period. The discussion is similar to the previous one, Each effect takes its own time.
Water and salt retention is a rather fast process (2-3 days), carbohydrates and potassium are slower, phosphorus is slower (months) and nitrogen is bound to even slower contractile proteins. Inhibition of spermatogenesis is completed in 3-5 months. Then “virilization” (apparently in children and women) occurs very slowly and, as you know, ends in years, not months. The concept of reversibility is also related to duration of action. Virilization is known to be almost irreversible; atherosclerosis is very small if caught early.
It follows from all this that medications, as a rule, should be taken in the shortest possible time necessary for building muscle proteins. Experience shows that a good anabolic effect is achieved after 4-6 weeks: at these doses, testicular atrophy and serum lipid modification are rather scarce.
The concept of dose is perhaps even more important in the case of low androgenic anabolic substances, which, as mentioned at the beginning are usually true at low doses. and they become more androgenic at higher doses. Using steroids that are too high and causing more side effects will only increase your risk of becoming “insensitive” to the drug itself. This phenomenon, typical of endocrinology, may be due to the fact that the cellular structures responsible for recognizing steroids and receiving the message of war (receptors) decrease in quantity if they are exposed for a long time to too high concentrations of the same, as to protect cells from overdose.
This phenomenon is called down-regulation (sub-regulation) and is also typical of thyroid hormones (beware !!!), insulin and other hormones ..
Well, many so-called drug formulators believe that switching from one steroid to another Is a method to eliminate downregulation.
You won’t believe that mother nature has created as many different types of receptors as steroids. on the market! There is only one steroid receptor, and if it decreases, the effect of any anabolic steroid will decrease. It also follows how wrong another typical bodybuilding practice is: stacking (using two or more steroids together) or even “bombarding” (megadoses of different drugs, type 100 deca, 200 testosterone, 200 primobolan … per day!): If the receptor ( poor fellow) only one, you put it only in your underwear.
Rather, it must be said that if the receptor is the same, this does not mean that different products have the same effect. In fact, once inside the cell, the steroid can be metabolized in different ways (I mentioned this earlier), causing different effects: c. for example, a more noticeable increase in phosphocreatine and mitochondria for a more androgenic (“massive” effect), a more noticeable increase in contractile proteins for a less androgenic (“power” effect), etc.
I advise you to re-read well what I wrote and keep this in mind. During steroid therapy (and even after its termination) it would be good to check at least the following indicators:
- pressure once a week
- Body weight every day (an increase of more than 1 kg per week is an undeniable indicator of water retention)
- A in the blood – SGOT, SGPT, Gamma-Gt, bilirubins, total cholesterol, triglycerides and HDL cholesterol (or protein electrophoresis).
- Every 3-6 months, especially if you are under strong androgen, you should have a rectal exam.
It is not advisable to bring these tests to your doctor unless he is an expert in the field and is friends with you.Look for a doctor who knows the environment and whom you trust to help you interpret the tests in light of the fact that you are taking steroids.
If, at last, side effects appear, what to do? I have to say this on an individual basis. However, in general I would say:
- If liver enzymes (SGOT, SGPT, Gamma-Gt or Bilirubin) change, stop using 17-alpha alkylates (Winstrol, Oxandrolone, Dianabol, etc.) and forget about them for the rest of your life. If you didn’t take them instead, it’s very likely that you have real liver disease, regardless of steroids.
- If you have a tendency to have low HDL cholesterol levels even in normal conditions and / or family members (dad, uncle, grandparents) with a history of heart attack, check this index very carefully and, if you really need to, do short cycles. Then try (but that’s even if you’re not on steroids) regularly aerobics throughout your life (that’s not what I’m talking about in terms of sports prevention, I’m not talking here).
- In the event of acne, avoid ignoring it until you become a leper. Miracles don’t work here, just: a) avoid using highly androgenic products and do not exceed therapeutic doses b) cleanse your skin properly and use antibiotic ointments (although acne, although androgens prefer them, is a bacterial infection) c) try to stay in the sun if it is possible.
- In the case of gynecomastia, you will almost always find testosterone or dianabol responsible. Well, all you can do is stop them and you won’t have to take any more flavored drugs.
- In the event of excessive (for your usual purposes) water retention, reduce the doses and you will see this phenomenon almost always subside. If this continues, be aware that there are other ways to reduce water retention, many of which are possibly worse than water retention ..
One more article is required for their exhaustive consideration, so I will only mention:
- Diuretics : they deplete salts, the effect is often uncontrollable, and if you really need to, use them for several days (and with appropriate supplementation) of minerals, which is strictly dependent on the diuretic or combinations of diuretics used). They can be very dangerous (if not for life, of course, for a sports presentation: consider doing weight or doing cramps racing …). However, diuretics were recently banned from IFBB racing.
- Antiestrogens : (tamoxifen or nolvadex, testonolactone and testolac, cyclophenyl). They are quite toxic drugs in the long run; they tend to give a slurry rebound effect (that is, when you stop them, you swell like balls), and this only acts on the estrogenic component of water retention anyway. Better not to use them at all. Their use can only be reserved for those who (often, even if they do not take anything) have really high estrogen levels (above 40 pg / ml, as confirmed by a blood test that still takes it) and suffer from delay
- Diet monitoring. Of course, if you limit the amount of carbohydrates, the delay disappears, but it doesn’t make sense if you are in the mass phase. Better to limit your sodium intake with a computerized diet: I say, limit, don’t rule out, because if you eat too little you will lose potassium, and even then you will have a blessed rebound (due to overproduction of the sodium-friendly hormone aldosterone ) and you would be very bloated like frogs if you eat food rich in salt. Instead of salt, limiting water intake, which is more than dangerous, is completely useless (the body sets up systems to retain even the small amount that you must take).
Finally, among natural systems, the most effective and beneficial is undoubtedly the regular practice of aerobic activities, such as running or cycling, which, unfortunately, almost no one does. Those who tend to suffer from retention should gradually practice aerobics (not dance!) And stay in training. It is not true that running makes you lose muscle; it only does so if, due to too low aerobic fitness (where you are, of course, if you are doing weights only), you increase your running doses too quickly.
And the last, the last word for women: I leave aside the debate about whether women should be muscular or rather flexible and slim (soft, tough, etc.). From a purely medical point of view, a woman who really wants to take an anabolic should definitely do it under the strict supervision of a specialist doctor (endocrinologist), since ultimately these are male hormones. In addition to the side effects associated with more or less pronounced masculinization, there is a risk of damage to all female functions (menstruation, possibility of pregnancy) due to their very delicate nature.