This article wants to stand out from the rest of the “Information” articles about AAS on the web. The web is full of articles on AAS and I personally have read several articles written by different authors and it would seem there is nothing to add here. Molecular characteristics, gene transcription and activity and receptor action of androgens have been considered very often; but this article is aimed at useful “additions”. All of the articles I’ve read on this topic are well written, but almost always contain the same information. Don’t get me wrong, all of the articles related to this topic are very helpful on an informative level, but when you finish reading them, they have almost nothing to “use” in the next cycle.
I’m sure you all know perfectly well what is the difference between oral and injectable AAS, but keep reading this article because I’m going to explain some things here that you could use in the next loop. In fact, I’m going to explain how you can use both oral and injectable Winstrol (stanozolol) and get completely different effects from the same molecule, depending on the route you choose.
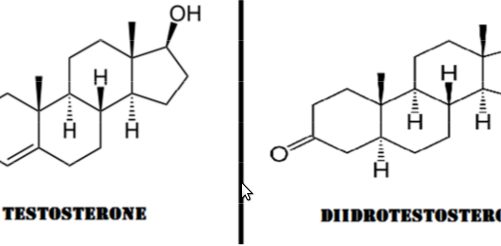
Structural differences between testosterone and dihydrotestosterone
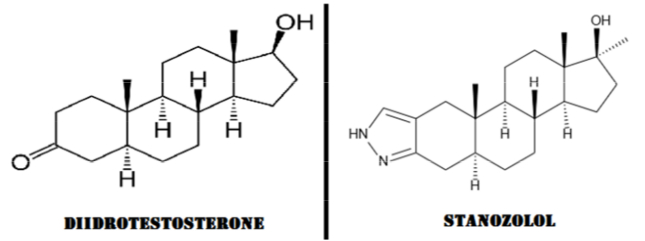
Winstrol (stanozolol) is a steroid derived from the basic structure of dihydrotestosterone (DHT).
Dihydrotestosterone (DHT) [full name: 5α-Dihydrotestosterone, abbreviated 5α-DHT; INN: androstanolone] is a biologically active metabolite of the testosterone hormone, formed mainly in the prostate gland, testes, hair follicles and adrenal glands under the action of the enzyme 5α-reductase with a decrease in the double bond between the 4th and 5th carbon atoms. DHT is also heavily involved in other characteristics commonly attributed to the male sex, including facial and body hair growth and voice depth. DHT can be inactivated in skeletal muscle by 3-alpha hydroxysteroid dehydrogenase and therefore has no significant effect on muscle hypertrophy. DHT has several beneficial effects that are more pronounced than the hormone from which it originates. DHT is able to increase the proliferation and activity of androgen receptors for almost 24 hours, and also has a profound effect on the central nervous system (CNS), which is why we often see a lot of aggression in athletes who use DHT derivatives such as Masteron (which has low anabolic value compared to androgenic). As an added benefit, DHT cannot aromatize (be converted by the aromatase enzyme) into estrogen.
Structural differences between dihydrotestosterone and stanozolol
___________________
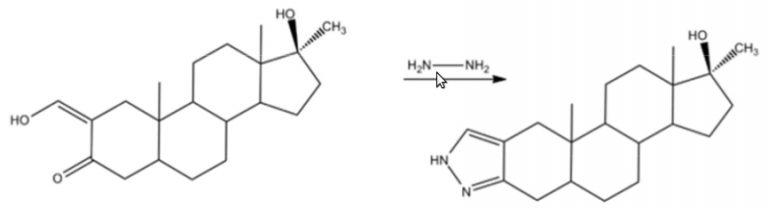 Image above: The “pyrazole” ring of Stanozolol can be obtained from oxymetholone by condensation of keto-aldehyde with hydrazine
Image above: The “pyrazole” ring of Stanozolol can be obtained from oxymetholone by condensation of keto-aldehyde with hydrazine
Oral Stanozolol (Winstrol)
When oral AAS is swallowed, it enters the stomach, where it is partially disturbed and carried into the small intestine. The small intestine contains a group of enzymes called CYP-450. These enzymes begin to destroy the AAS even more in an attempt to deactivate it. The AAS is then absorbed through intestinal mucosal cells and transported into the hepatic portal vein for further deactivation with chemicals such as etiocolanone. These chemicals are then combined with glucuronic acid and excreted in the urine. This process, known as first pass deactivation, can deactivate up to 100% of the original material. By altering the molecular structures of the AAS, deactivation can be significantly reduced. Some AAS become orally active by adding an alkyl (methyl or ethyl) chemical group to the alpha position of the 17th carbon atom: these AAS are commonly referred to as C17-alpha alkylated or methylated (as is the case with oral Winstrol). This change, which is present in Winstrol, is performed in such a way that more of the molecule enters the bloodstream and remains active for a long period. It is important to note that the molecule passes a second time through the liver through the portal vein and then finally returns to the bloodstream through the hepatic vein. The liver is a filtering element of the body and removes a large amount of dangerous toxins and other substances from the blood.
So, as you can see, when you take an oral c17 steroid like Winstrol, it undergoes first-pass metabolism in the intestines and liver. Some drugs can be absorbed more or less completely intact after moderate metabolic activity, and some only after intense metabolic activity. The drug now travels further away from the liver, where it undergoes what is called second-pass metabolism. Of course, in the case of Winstrol, an injectable version is available, and when we compare the oral and injectable versions of Winstrol and its effects on the body, we find some surprising differences. The injectable version (naturally) goes directly into the bloodstream and undergoes only a much less violent activation of the second metabolic pathway, while the oral version, as previously shown, must go through two liver passages before finally entering the circulation.
Stanozol (Winstrol) for injection
Now, here’s the fun part: when you inject Winstrol instead of taking it orally, you can get greater nitrogen retention, especially at the topical injection level (and therefore more muscle growth). Therefore, if you are trying to use Winstrol to build new muscle tissue, especially locally, the injectable version appears to be far superior to the oral version. However, the oral version has some advantages over the injectable version, including possible synergy with other drugs, but only (mostly) orally.
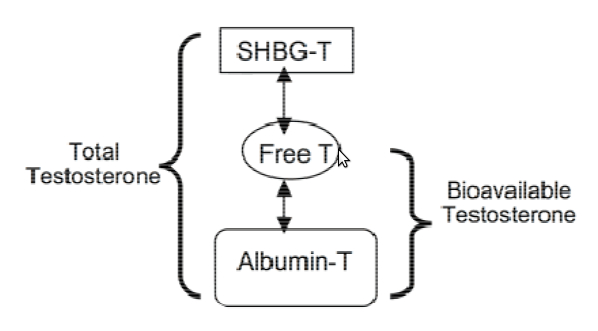
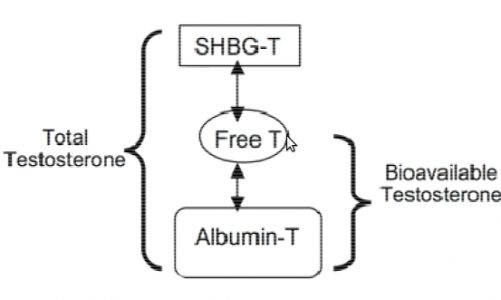
In the liver, during the first passage, Winstrol is exposed to various enzymes and proteins. To understand how the synergy between Winstrol and other steroids (mentioned earlier) is possible, we need to understand what a “ sex hormone binding globulin” is. “(SHBG). For our purposes here, all we need to know is that SHBG is a glycoprotein made in the liver that binds to testosterone, transporting it into the bloodstream in the body. Therefore, SHBG is used to transport testosterone and other AAS throughout the body, but as long as the link is maintained, the testosterone / AAS molecule cannot have anabolic effects.
Of the testosterone produced endogenously by the body, approximately 97-99% is contained in bound form and is therefore inactive, although free, and therefore active testosterone is equivalent to 3-1% of total testosterone. This may not sound like much, but 0.1-0.3 mg of free testosterone also contains many distinct individual molecules, and the molecule can activate androgen receptor sites multiple times.
As mentioned earlier, Winstrol has the ability to reduce SHBG production in the liver on average by 60%. A relatively low dose of oral winstrol of 0.2 mg / kg / day has been shown to reduce SHBG by almost 50%. For a hypothetical 100-pound Bodybuilder, it would take as little as 20 mg / day to cut circulating SHBG in half and increase active testosterone / AAS. It is logical that with less circulation of SHBG the cycle of anabolic steroids will be more efficient.
– But why can we expect such a sharp decrease in SHBG only with oral Winstrol? –
Since the effect of Winstrol is used in the phase of the first passage of the liver, it is much more acute, where SHBG is synthesized.
Looking at the study comparing injectable contraceptives with the oral version, we see that the oral version at 70 mg / week (10 mg per day orally) is more effective at affecting SHBG levels than 400 mg per week. to inject! In this study, testosterone undecanoate was administered at a constant dose with noresisterone (which increases SHBG). What is known is that when norestisterone is administered orally, it causes an increase in SHBG compared to when it is administered by injection. And this also happens when the doses of the injectable drug are 4 times higher! Of course, in this study, it is obvious that the interaction with SHBG of the oral version with respect to the injectable version is more pronounced with the introduction of the first (oral compound) than with the second (injectable).
Thus, by injecting a small amount of oral winstrol during a cycle, reducing SHBG, we will create an environment in which more of the other AAS co-administered during the cycle will be in a “free” state and therefore active.
Lately, many trainers have been recommending that athletes use the injectable version of Winstrol instead of the oral one.
The reason these trainers recommend women to avoid the oral version of this product is the same as for men who believe it gives them more synergy and effectiveness in their cycles.
When SHBG decreases in women, more free testosterone appears in the blood. And as we’ve seen, the oral version of stanozolol negatively affects SHBG more than the injectable version. When we lower SHBG levels in women too much, we notice a strong correlation with the appearance of hyperandrogenism and hirsutism (abnormal growth of body hair). In addition, low SHBG levels in women contribute to menstrual irregularities.
Finally, and (partly) anecdotally, we also note a higher incidence of clitoris enlargement and acne enlargement when women use the oral version of Winstrol. instead of injection. The reasons for this are obvious: when we increase free testosterone by lowering SHBG, we increase the amount of testosterone, which can be reduced by 5a to DHT. DHT is the main culprit in acne and also the hormone responsible for the enlargement of the external genitals. It is clear that it is for this reason that we see higher rates of clitoral hypertrophy as well as acne when oral Winstrol is used by women.
We can also observe an increase in acne when men use Winstrol orally, but these effects are relatively limited when a dose of 0.2 mg / kg is administered to increase the effectiveness of other AAS in a single cycle. This is, of course, no excuse for using Winstrol for an extended period of time. As mentioned earlier, stanozolol has one of the highest liver toxicity (hepatotoxicity) among the oral doses of AAS per mg. Not to mention its pronounced deleterious effects on the lipid profile (cholesterol), even at low doses.
Finally, the reader will understand that oral Winstrol can be used in any cycle to increase its effectiveness, but should be used sparingly because of its hepatotoxicity and ability to alter the lipid profile. When used in cycles based on testosterone (or other SHBG-related AAS), a dose that will halve SHBG levels can increase the effectiveness of other AAS. Oral Winstrol also has the added benefit of causing an increase in IGF-1 production in the liver in response to first-pass deactivation. This is the case for all C-17 alkylated oral AAS.
When taken as an AAS to increase muscle mass, the recommended oral doses of stanozolol for men are usually 20-30 mg per day (although 30-50 mg per day has been shown to be much more effective, but also more toxic) and 10-15 mg for women. Usually, however, a 20-30 mg / day oral dose of stanozolol (and even more if the dose reaches 50 mg / day) is quite expensive (especially if the drug is pharmaceutical / veterinary), which is why some athletes use the injectable version (as mentioned earlier , very similar to oral) oral ingestion of a prefixed dose: Swallowing 0.5 ml of the classic injectable version of Winstrol Desma is equivalent to taking 25 mg of oral stanozolol. The active life of the oral form of stanozolol is 8-9 hours; It follows that administering a daily dose divided into two to three portions is the best approach.
Injectable Winstrol has proven to be the best choice when you want maximum localized protein synthesis. In the course of my research, I have found that AAS injected directly into the muscle belly (especially if it is a “small” muscle group) enhances local growth.
There are mainly two factors involved:
- The local availability of any fast / short acting substance causes a greater localized stimulus to the receptor sites of the cells. Given that local injection protocols are followed in the muscles retained, this effect is likely also due to the fact that these groups are subject to less blood flow and nutrient carryover. This is often associated with inadequate development of vascular and neural factors in these areas.
- Local injection protocol theory states that when a filling is inserted, the muscle fibers and fascia are forced to stretch and enlarge. This, in turn, creates localized growth due to more space available for cell and muscle fiber hypertrophy.
However, the most effective AAS for local injection protocols are unesterified ones such as injectable Winstrol. Since esterified AAS are highly dependent on the conversion of the esterase enzyme to their active ester, and since there is not much esterase at the point of intramuscular injection, there is less local stimulation of the cell receptor sites. There is no problem with unesterified AAS, and their local anabolic effect is noted. This is why injectable Winstrol is often used during pre-race cycles as part of a local injection protocol in retained muscles or to enhance muscle quality and streaks at specific points, such as between the deltoid muscle and the ribcage.
Recommended doses of stanozolol for injection are typically 50-100 mg every 1-2 days: when applied topically, the dose can be divided into 1 ml (50 mg) administered to the remaining muscle group, for a total of 100 mg. Women usually use injectable doses of stanozolol 25-50 mg per week or 25 mg 2-3 times a week.
Liver toxicity for Winstrol injections is slightly lower (mg x mg) than oral, but nevertheless present and not insignificant ( this also applies to the ability to alter blood lipids). There have been discussions for a long time about the active life of injectable Winstrol, of which there are a variety of estimates, understandable on the basis of a rather subjective concept of active life, but also regarding the very different sizes of microcrystals in which Winstrol is in solution: the crystals are wider the longer the active life. The “fastest” drug currently available is the unesterified oily drug, which is starting to appear in various UGS laboratories.
In conclusion, we can say that the two versions of Winstrol (oral and injectable) are identical, but they have single and proper qualities. in each (for example, a decrease in SHBG in the oral version or an increase in localized growth in the injectable version). If doses are carefully calibrated and calibrated, both options can be used in the same cycle, using the unique characteristics of each.

